
On January 30, 2025, the U.S. Food and Drug Administration (FDA) approved the drug Journavx™ (suzetrigine), a first-in-class nonopioid analgesic to treat moderate to severe pain in adult patients.1 The Acting Director of the FDA’s Center for Drug Evaluation and Research, Jacqueline Corrigan-Curay, MD, JD, called the approval “an important public health milestone in acute pain management…an opportunity to mitigate certain risks associated with using an opioid for pain and provides patients with another treatment option.” Suzetrigine is the first drug to be approved in a new class of pain management medicines. Despite approval of numerous analgesic agents throughout the 20th century, greater than half of surgical patients still experience moderate to severe postoperative pain.2
Suzetrigine, a nonopioid, nonaddictive, selective pain signal inhibitor, holds the potential to be the first treatment for moderate-to-severe acute pain in a new pharmacologic class in over two decades. Suzetrigine inhibits NaV1.8 by binding to the protein’s second voltage sensing domain (VSD2) to stabilize the closed state of the channel. This novel allosteric mechanism results in tonic inhibition of NaV1.8 and reduces pain signals in the primary human dorsal-root ganglion (DRG) sensory neuron. By blocking pain signals in nociceptive C-fibers, before they reach the brain, suzetrigine offers an alternative to opioids without addiction or organ toxicity.
Acute, neuropathic, or inflammatory pain is caused by excessive firing of dorsal-root DRG or trigeminal ganglion neurons. The identification of multiple sodium channel genes led to a search for “peripheral” sodium channels essential for DRG neuron firing but not involved in the brain or heart. Three such channels—NaV1.7, NaV1.8, and NaV1.9—regulate peripheral pain-signaling in nociceptive C-fibers. Of these three channels, NaV1.8 produces more than 70% of the current, allowing propagation of the action potential. Suzetrigine inhibits depolarization in peripheral pain-signaling neurons without an effect on the brain or heart, thereby reducing pain with few central nervous system (CNS) or cardiac side effects. In vitro studies show suzetrigine has a >31,000-fold selectivity for Nav 1.8 channels, unlike nonselective sodium channel blockers.3 Suzetrigine specifically and solely targets the NaV1.8 receptors, avoiding unpleasant side effects (Figure 1).4 Future NaV1.8 molecules may offer even greater analgesic potential pending clinical trials (Figure 2).
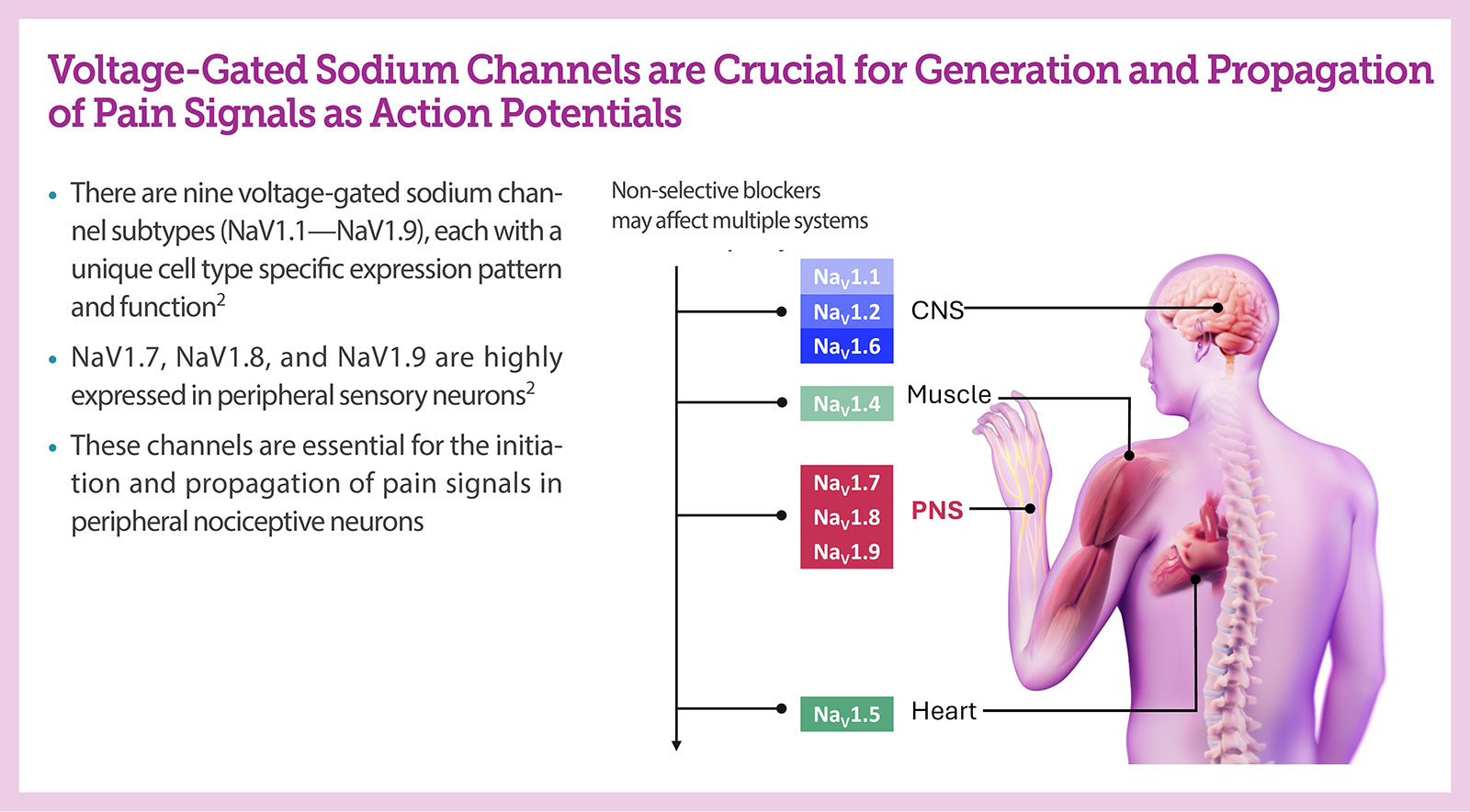
Figure 1: Voltage-gated sodium channels associated with the propagation of pain signals. Used with permission from Vertex Pharmaceuticals.
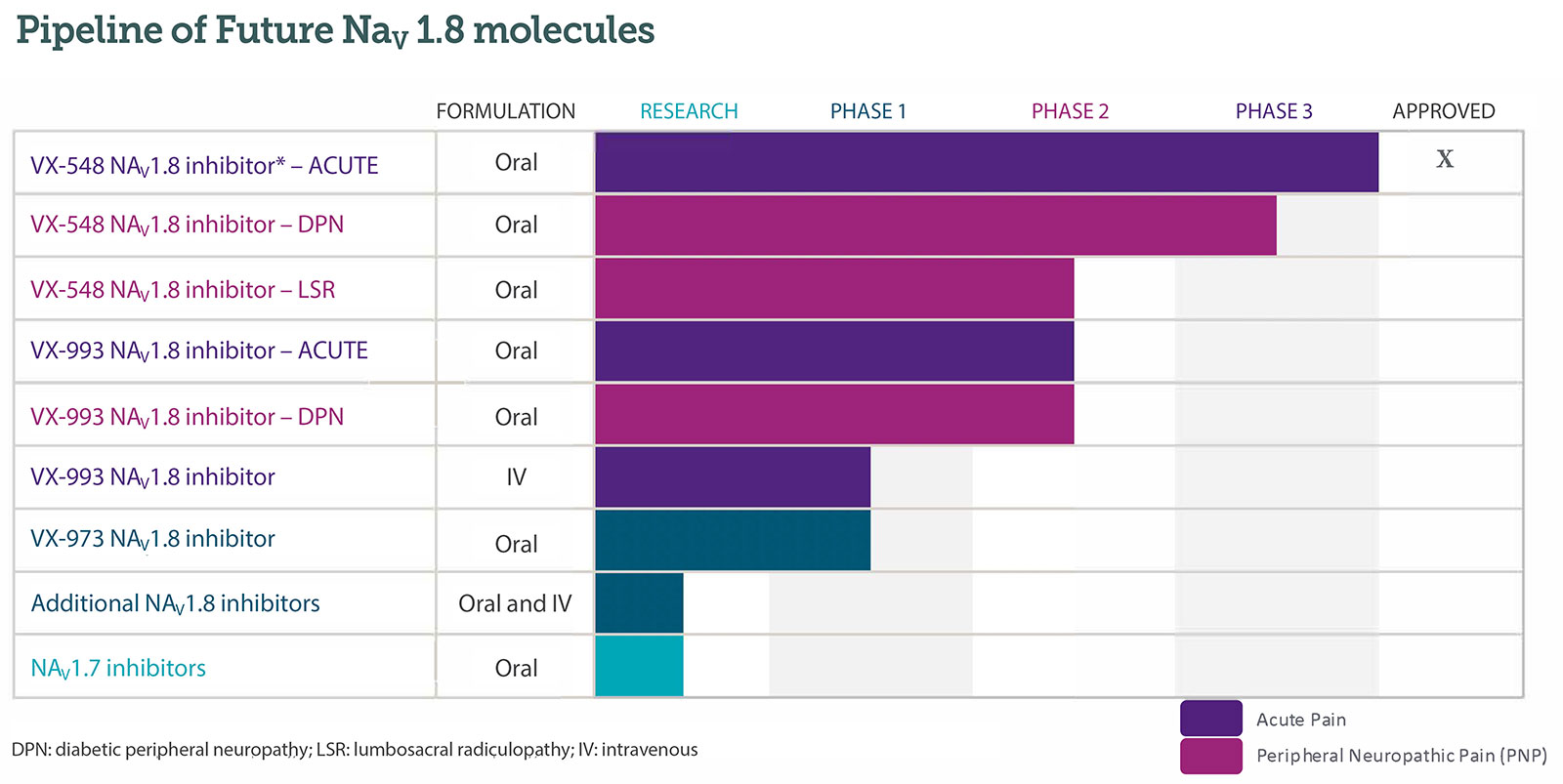
Figure 2: Pipeline of future Nav1.8 molecules. Used with permission from Vertex Pharmaceuticals.
To test drug safety and efficacy, Vertex Pharmaceuticals (Boston, MA), conducted two large randomized clinical trials: an abdominoplasty trial that enrolled 1,118 patients and a bunionectomy study with 1,073 patients. Patients were randomly assigned to one of three groups: a placebo, a combination of acetaminophen and hydrocodone, or suzetrigine. The recommended loading dose of suzetrigine is 100 mg orally, followed by 50 mg every 12 hours.1 In addition to receiving the randomized treatment, all participants in the trials who experienced breakthrough pain were permitted to use ibuprofen as needed for “rescue” analgesia. Both trials demonstrated a statistically significant superior reduction in pain with suzetrigine compared to placebo. Superiority versus the combination of hydrocodone 5 mg/acetaminophen 325 mg was not demonstrated. However, a responder’s analyses at various timepoints (12h, 24h, and 48h) showed similar 30/50/70% reductions in Numeric Pain Rating Scale of suzetrigine versus hydrocodone 5 mg/acetaminophen 325 mg. Side effects of suzetrigine reported by patients were similar to those taking the placebo. There may be an increased risk of adverse reactions with the concomitant use of moderate to strong CYP3A inhibitors. There may also be a risk of drug interactions with certain hormonal contraceptives, and patients taking suzetrigine should use nonhormonal contraceptives (such as condoms) or use alternative contraceptives containing levonorgestrel and norethindrone.
Patients with moderate to severe hepatic impairment may have higher systemic exposure of suzetrigine and its active metabolites. Suzetrigine should be avoided in patients with renal impairment of eGFR < 15 mL/min.
The most common adverse reactions in study participants who received suzetrigine were itching, muscle spasms, increased blood level of creatine phosphokinase, and rash. Suzetrigine was generally safe and well tolerated with a lower incidence of adverse events than placebo and the acetaminophen/hydrocodone combination. Additionally, patients should avoid food or drink containing grapefruit when taking suzetrigine.
Sodium channel inhibitors might be able to fill the unmet need in perioperative pain management with current nonopioid analgesics. Postoperative pain control is a vital component to proper recovery for surgical patients. One major component of successful programs such as Enhanced Recovery After Surgery (ERAS) protocols is optimizing pain control throughout the entire perioperative period. This starts with preoperative loading of acetaminophen and ibuprofen, which acts synergistically with other analgesics. Intraoperatively, postoperative pain is minimized with regional anesthesia blocks and catheters. Suzetrigine appears to be an effective, safe, and nonaddictive medication that can provide new options for patients at high-risk of opioid-related adverse events or where nonsteroidal anti-inflammatory drugs (NSAIDS) are contraindicated, offering a meaningful alternative to opiates with ERAS protocols.
The FDA approved suzetrigine on January 30, 2025, for the oral treatment of moderate to severe pain. Suzetrigine is a selective sodium channel blocker and is the first sodium channel blocker to be approved in the United States for this indication and is the first nonopioid drug to be approved for the treatment of pain in over 25 years. Suzetrigine is a selective blocker of the voltage-gated sodium channel NaV1.8 which is expressed in peripheral dorsal root ganglion neurons. Suzetrigine has no abuse potential and no known organ toxicity; therefore, it is a reasonable alternative to opiates or NSAIDs.
REFERENCES
- FDA approves novel non-opioid treatment for moderate to severe acute pain—press release: January 30, 2025. https://www.fda.gov/news-events/press-announcements/fda-approves-novel-non-opioid-treatment-moderate-severe-acute-pain. Accessed March 28, 2025.
- Van Boekel R, Warle M, Nielsen R, et al. Relationship between postoperative pain and overall 30-day complications in a broad surgical population: an observational study. Annals of Surgery. 2019:269:856–865. PMID: 29135493.
- Osteen JD, Immani S, Tapley TL, et al. Pharmacology and mechanism of action of suzetrigine, a potent and selective NaV1.8 pain signal inhibitor for the treatment of moderate to severe pain. Pain Ther. 2025;14:655–674. PMID: 39775738.
- Waxman SG. Targeting a peripheral sodium channel to treat pain. N Engl J Med. 2023;389:466–469. PMID: 37530829.