
Author: Micheal Vlessides
Anesthesiology News
Optimizing OR management has been the focus of exhaustive research. But one subject that has yet to be analyzed is maximizing OR productivity and safety in the COVID-19 era, when a shortage of personal protective equipment (PPE) is the defining variable.
However, in a recent article in Anesthesia & Analgesia 2020 Mar 26. Franklin Dexter, MD, PhD, and his colleagues explained some of the principles behind this type of OR optimization.
“Hundreds of papers have studied operating room management, in which there are different types of constraints, but there has not been a single paper written in which the binding constraint is the amount of PPE,” said Dr. Dexter, a professor of anesthesia at the University of Iowa, in Iowa City.
The primary objective of the research, Dr. Dexter said, was achieving the lowest possible infection risk while caring for patients with unknown COVID-19 status at the time of anesthesia. The recommendations assume institutions are only performing essential surgeries during the pandemic.
4 Strategies
Longer Shifts
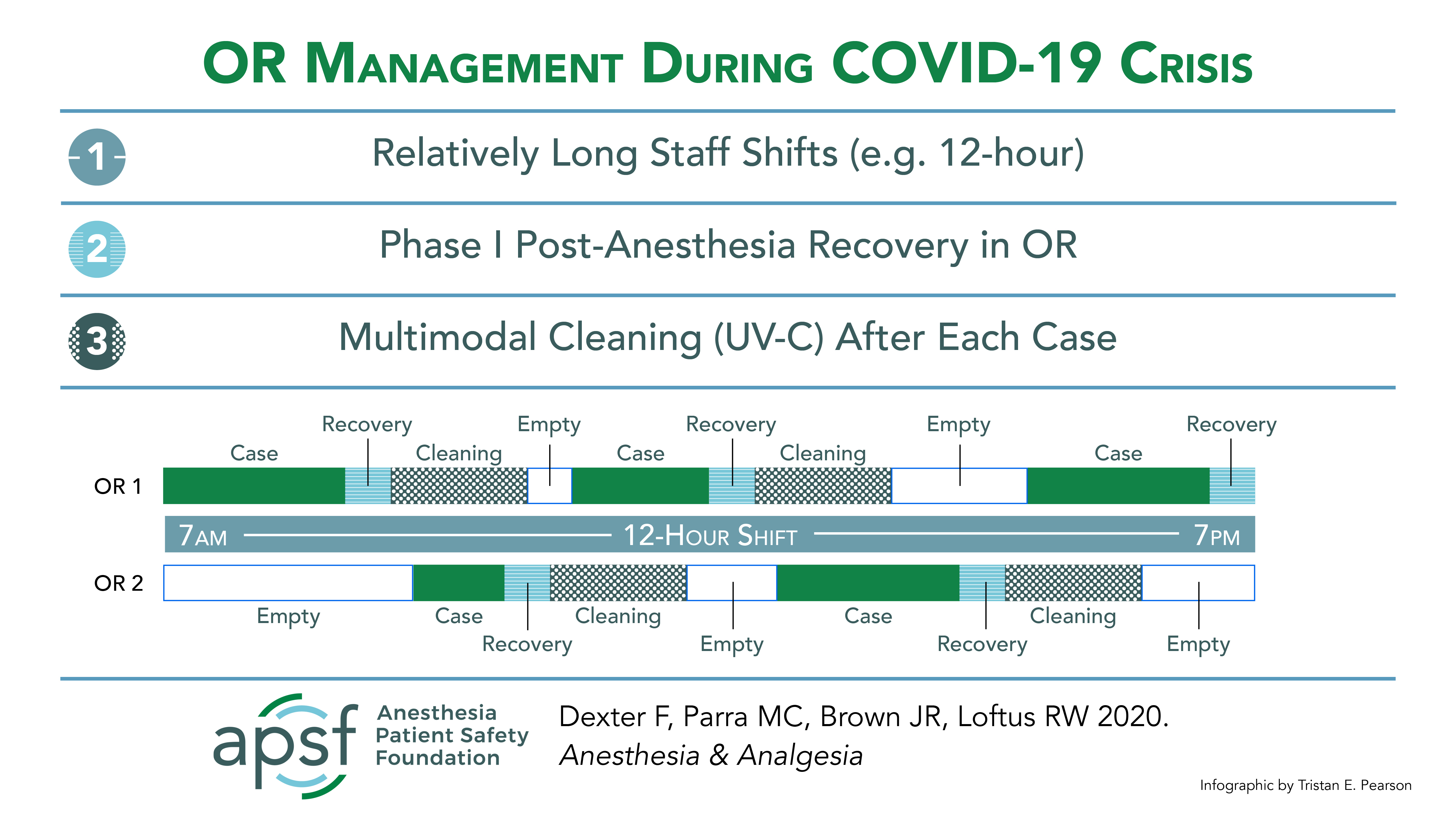
With that in mind, he and his colleagues suggested four primary strategies, beginning with the use of relatively long (such as 12-hour) staff shifts, which they believe will reduce the use of protective masks, the potential for COVID-19 exposure, and the number of clinicians interacting with patients.
“Since a person can wear a surgical mask throughout the day, this will reduce the number of surgical masks used,” Dr. Dexter told Anesthesiology News.
As part of that strategy, they recommended the use of fewer surgical teams completing more procedures. For example, an institution might have eight essential cases to perform (each lasting one or two hours) in eight ORs sharing one master ventilatory system.
In a traditional approach, the eight first-case starts would take place in eight ORs with eight different teams of providers. In the PPE shortage scenario, however, the suggested approach is to have two teams complete all eight cases in available rooms. This, the investigators noted, sees fewer personnel exposed to patients who may or may not be infected.
Thorough OR Cleaning and Limited Use
Second, the authors recommended that only one case be performed in each OR daily. This will afford institutions the opportunity to clean each room thoroughly during the pandemic, including terminal cleaning with the addition of ultraviolet-C light.
“Because of the false-negative rates with COVID-19 testing, we need to proceed as though all patients are infected,” Dr. Dexter explained. “That’s why we recommend this multimodal—‘terminal’ or ‘deep’—cleaning after each case.
“Although it takes quite a bit of time, it wouldn’t affect throughput, because the number of available operating rooms is very large, as we’re limited by the amount of personal protective equipment.”
No PACU Recovery
The authors’ third recommendation was that patients do not go into a large, pooled phase 1 PACU after surgery, as this would both increase the risk for contamination and use precious surgical masks. Instead, they suggested that most patients recover in the OR where they underwent surgery (Figure).
“Recovering the patient in the operating room is the norm in countries such as Japan,” Dr. Dexter explained. Of note, previous research (Can J Anaesth 2018;65[12]:1296-1302) has found that time to patient recovery in a Japanese hospital was significantly faster than at Dr. Dexter’s institution.
“The amount of time the patient stays with the anesthesiologist is much briefer than at hospitals where the patients go to a phase 1 recovery room with nursing protocols,” he added. With this in mind, they also recommended that clinicians consider the use of anesthetic drugs that reduce recovery times.
Finally, the authors recommended improved communication as a way to maintain throughput while minimizing potential coronavirus exposure. For instance, if a surgeon is scheduled for only one procedure later in the day, he or she can be notified by the anesthesia or nursing teams when closure begins on the preceding case. Such communication, they explained, will reduce total exposure time in the OR, but should not limit workflow as long as the preceding patient recovers in the OR.
“This will still give the surgeon enough time to get to the surgical suite to change and prepare,” Dr. Dexter said.
Despite these recommendations, Dr. Dexter and his colleagues hope they soon become obsolete as the supply of PPE ramps up to meet current demand.
“This is clearly a temporary measure,” he noted. “Hopefully in six to eight weeks, everything we did here will no longer apply. And that’s OK.”