
Summary:Pediatric anesthesia safety has improved markedly over the past four decades through advances in monitoring, pharmacology, airway management, and safety culture. Ongoing challenges include perioperative risk in neonates and infants, medication safety, neurodevelopmental concerns, and global disparities. Future priorities focus on simulation, data-driven practice, and equitable worldwide access to safe pediatric anesthesia.
KEY POINTS:
- Mortality and major complications in pediatric anesthesia have declined with pulse oximetry, capnography, and standardized monitoring. >>
- Airway management and drug safety remain central safety concerns, especially in neonates and infants. >>
- Research continues on anesthetic neurotoxicity and long-term neurodevelopmental outcomes. >>
- Global disparities in pediatric anesthesia safety require international collaboration and resource development. >>
- Future directions emphasize big data, precision medicine, and equity in care delivery. >>
Shortly after the introduction of anesthesia for dental and surgical procedures in the 1840s, the death of a 15-year-old girl during chloroform anesthesia precipitated a focus on safety in pediatric anesthesia.1 Pediatrics was quickly recognized as a distinct discipline in anesthesiology by John Snow, anesthesiologist, epidemiologist, and author of the earliest anesthesia textbooks.2,3 The diversity of the pediatric population in terms of age, weight, anatomy, and psychosocial disposition could present many safety challenges; children were not simply “little adults.” From history to present day, there is ample evidence for safety as a principal concern in pediatric anesthesia.
HISTORICAL INNOVATIONS IN PEDIATRIC ANESTHESIA
The historical safety innovations in pediatric anesthesiology over 30-year periods are summarized in Table 1.4-7 Innovations can be grouped by technology (e.g., hardware, software, drug), people (e.g., education, technique), or organization (e.g., professional society, operating procedure). Many innovations seen in pediatric anesthesiology were modified and customized from adult practice, since the earliest pediatric anesthesia practitioners were dentists, surgeons, and general anesthesiologists. More recent pediatric innovations resulted from the evolving field of safety science. “Wake-Up Safe,” the patient safety organization of the Society for Pediatric Anesthesia (SPA), has collaborated with the Children’s Hospital Association’s “Solutions for Patient Safety,” the Institute for Healthcare Improvement, and the United Stated Navy, as one such example.
Table 1. Pediatric Anesthesia Safety Innovations by Period.
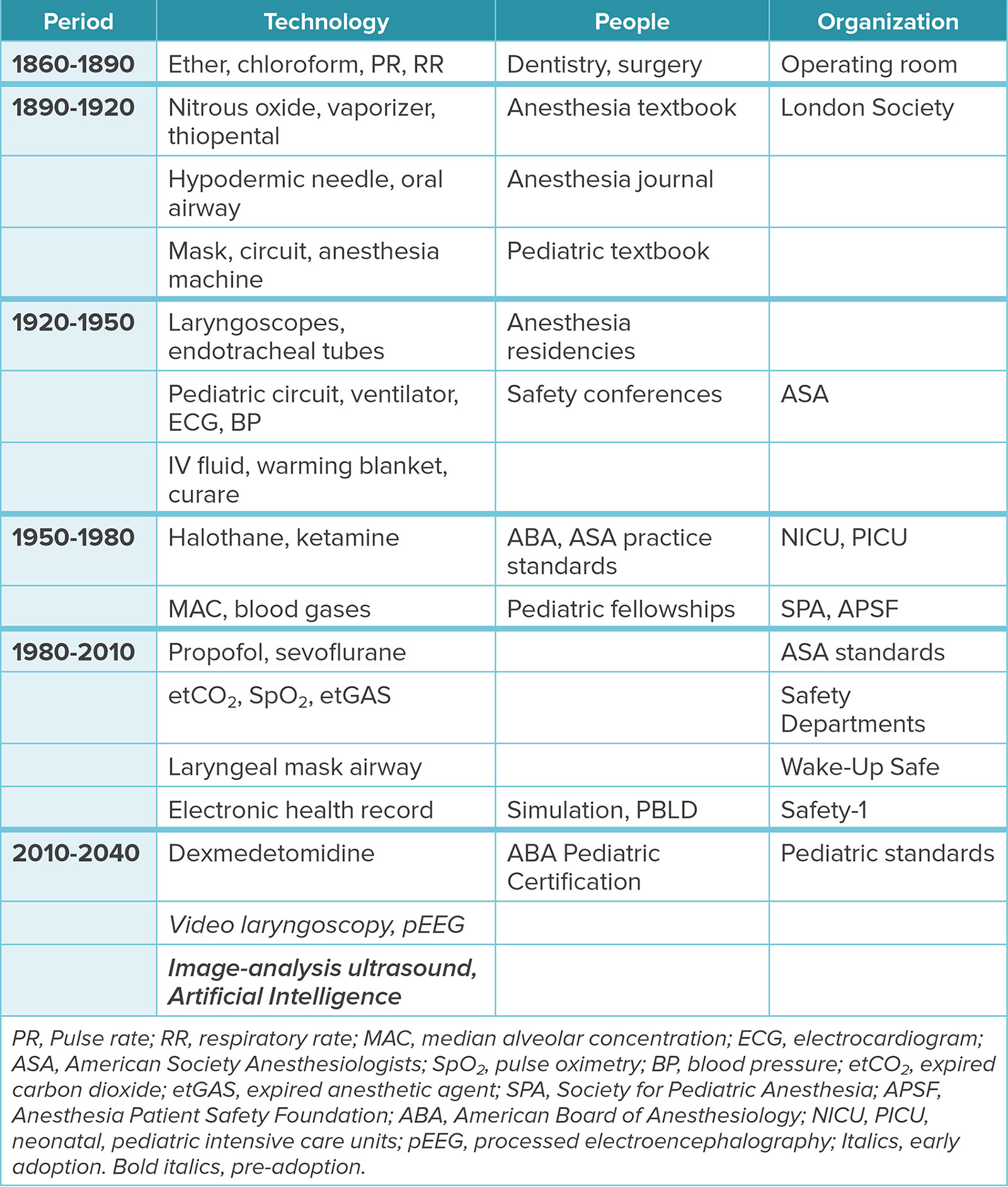
At the beginning of pediatric anesthesia practice, inhalation of ether or chloroform through a face cloth or inhaler was used to induce children and adolescents until unconsciousness and immobility ensued. Neonates and infants did not receive anesthesia. The monitoring of respiratory and heart rate in the operating room (OR) was a notable innovation in safety at this time. During the early 1900s, anesthesia machines containing bag, circuits, mask, oxygen, nitrous oxide, and vaporizers were invented, which undoubtably improved pediatric anesthesia safety. The earliest anesthesia professional emerged as a separate medical specialty from surgeons and dentists during this period.
The years between 1920–1950 witnessed many innovations. The first pediatric anesthesia textbook, Anesthesia in Children, was published in 1923.8 Although hypodermic needles, thiopental, blood pressure cuffs, and electrocardiogram (ECG) monitors were available, they were rarely used in pediatrics until the 1930s, when Dr. William Ladd at Boston Children’s Hospital founded the subspecialty of pediatric surgery, and infant anesthesia was first attempted for major procedures like correction of intestinal malrotation and tracheoesophageal fistula.9 The addition of ventilators and curare during the 1940s fostered invention of pediatric-sized laryngoscopes, endotracheal tubes, intravenous fluids, and warming blankets for pediatric anesthesia. Most neonatal and infant anesthetics in the 1940s and 1950s were performed with mask anesthesia or using custom made tracheal tubes, because the cuffed rubber endotracheal tubes used in children and adults could not be manufactured for the small size of neonates and infants. Hemodynamics were assessed by ECG, pulse, and precordial sounds. Educational and organizational innovations included anesthesiology residencies with specialty rotations in pediatric care, mortality conferences, and the founding of the American Society of Anesthesiologists (ASA) to educate best clinical practices. Pediatric perioperative and anesthesia-
related mortality from 1947–1956 declined, from 49 to 29 cases per 100,000.1,5
Innovations in pediatric anesthesia safety from 1950 to 1980 enabled surgery on younger and sicker patients. Halothane, a nonflammable vapor, permitted electrocautery, which allowed for a broader range of surgical procedures to be performed, such as cardiovascular, thoracic, and major abdominal surgery. Determination of minimum alveolar concentration and greater precision in vaporizer delivery improved dosing of volatile anesthetics in children. Creation of neonatal and pediatric intensive care units (NICU and PICU) in the 1950s and 1960s, respectively, allowed for improved postoperative monitoring and care for neonates and infants. In the 1960s, neonatal and infant plastic endotracheal tubes became commercially available, and in the 1970s, mechanical ventilators and arterial transducers were developed for use in the NICU. These advances, along with use of ketamine as an alternate anesthetic to halothane, enabled more surgery on neonates, infants, and sicker patients. In response to rising acuity, the ASA developed the physical status score for risk stratification, pediatric anesthesiology fellowships were developed, and hospitals began to require privileges for the practice of pediatric anesthesia. Pediatric anesthesia-related mortality decreased by two-fold from the prior 30 years to 8 per 100,000 cases during this period.5
Between 1980–2000, patient acuity and surgical complexity increased even further. Sevoflurane and propofol, possessing less cardiovascular depression and airway reactivity, replaced halothane and thiopental in the 1990s. Pulse oximetry, capnography, and expired sevoflurane monitors permitted real-time assessment of anesthetic drug level, oxygenation, and ventilation to better detect hypoxia, hypoventilation, and anesthetic overdose. Anesthesia machine ventilators for neonates also became available in the 1990s. Automated blood pressure devices entered the market, allowing for frequent blood pressure monitoring, and replacing manual blood pressure measurements and reliance on precordial stethoscopes. Laryngeal mask airways became available to mitigate difficult airway events and pediatric anesthesiologists began using cuffed endotracheal tubes as concerns regarding tracheal cuff pressure injuring the subglottic area were diminished. ASA practice standards, the Society for Pediatric Anesthesia (SPA), and the Anesthesia Patient Safety Foundation were created, which educated and influenced pediatric anesthesia professionals to follow the safest practices. Collectively, these innovations were associated with decreases in pediatric perioperative and anesthesia-related mortality to 24 per 100,000 cases and 4 per 100,000 cases, respectively, 2–5-fold less than the previous era.5
Since 2000, many safety innovations have involved education and organization, rather than technology. The Institute of Medicine’s Report “To Err is Human—Building a Safer Health System” pushed hospitals and professional organizations to adopt safety science and specifically utilizing the Safety-1 framework, consisting of education, creation of pediatric standards and safety departments, and implementation of electronic health records (EHR).4,10 The use of EHR enabled the development of databases, analytics, metrics, look-up tables, checklists, and critical notifications as tools to promote perioperative patient safety. Important pediatric anesthesia innovations in this safety domain include the SPA’s “Wake up Safe,” a federally sanctioned patient safety organization composed of 75 pediatric anesthesia departments, which offers education in tools such as safety analytics and quality improvement.1 Additionally, in collaboration with the American College of Surgeons, the SPA established quality standards for pediatric perioperative care during this period.11,12 The American Board of Anesthesiology also approved a special certification for pediatric anesthesia. By 2015–2019, pediatric perioperative and anesthesia related mortality decreased to 11 per 100,000 cases and 0.5 per 100,000 cases, respectively, 2–5-fold less than the previous era.7,11
PEDIATRIC ANESTHESIA SAFETY: WHAT’S NEXT
Looking forward to the next 10 years, the workload for pediatric anesthesia professionals will continue to grow due to higher-acuity patients and more complicated procedures.13 Further, half of current pediatric anesthesiology fellowships remain unfilled, leading to concerns about a shortage of trained anesthesia professionals to care safely for these complex patients. To counter the potential for an increase in adverse events, additional innovations will be needed. Future innovations should be directed toward prevention of nonfatal adverse events, such as airway and cardiopulmonary events, which occur more often (0.1–5.2%) in neonates, infants, ASA physical status 3–4 patients, and in patients undergoing major surgery.7,10
Video Laryngoscopy (VL)
VL can help improve the reliability of first attempt intubation in neonates, infants, and children with difficult airways, as repeated attempts are common causes of hypoxia and cardiac arrest in this population. VL improves reliability of intubation due to a brighter, larger view of the larynx, and a video screen that allows other clinicians to assess the anatomy and verify intubation. VL also enables a learner to practice intubation with an educator to teach airway anatomy and intubation skill better than direct laryngoscopy (DL). Neonatal airways pose a challenge for learners, as well as experienced clinicians, due to the limited space of the oropharynx to place the laryngoscope blade, view the anatomy, and insert the endotracheal tube before desaturation. The use of VL in neonates and infants has been shown to increase successful first-attempt intubation rates, along with fewer desaturation and cardiovascular events.14 In pediatric anesthesiology, VL is standard practice in a few departments, clinician-dependent in most departments, and not available in other departments.
Intensive Care and Emergency Units have more rapidly adopted VL than pediatric anesthesiology, and it has become common for teaching in these specialties.15 Successful first-pass DL intubation rates are often lower in these specialties than in pediatric anesthesiology, and failed intubation in critically ill children more often results in adverse events than in healthy children undergoing elective surgery. The main barriers to adoption of VL in pediatric anesthesiology are change in practice and training from DL, cost of VL in all anesthetizing locations, and sustainability, as VL often utilizes disposable blades.
Image Analysis Ultrasound
Ultrasound can help improve the diagnosis of causes of hypotension, low cardiac output, and poor ventilation in the OR, and facilitate vascular access. Computer-generated image analysis of ultrasound is currently used in radiology; ultrasound machines can deploy image analysis using artificial intelligence (AI), which can assist with structure identification and needle placement, while providing real-time feedback for the clinician and trainee.16,17 Such AI-assisted technology may be especially helpful for anesthesia professionals inexperienced and unpracticed in ultrasound.
The continued improvement of ultrasound technology, with higher resolution and reduced image artifacts, is enhancing anesthesia professionals’ skills in vascular access, regional anesthesia, Point of Care Ultrasound (POCUS), and cardiovascular assessment. Yet in neonatal and pediatric patients, these technical procedures remain challenging due to small size of structures, variable anatomy, infrequent use of the technology, and challenges with scalability of AI-assistance. This results in multiple attempts, failed diagnoses, and potential complications. Further, many anesthesia professionals trained prior to widespread adoption of ultrasound, and efforts for national and institutional education should be increased.
Barriers to adoption of image analysis ultrasound in pediatric anesthesiology include the lack of education and exposure to the technology, high cost (including purchasing and maintenance), as well as the large size of the machines in small ORs. While many portable ultrasound probes have been developed for adult patients, scalability may present a challenge.
Gastric Ultrasound and Fasting
The debate surrounding preoperative fasting has gained renewed attention with the rise of Glucagon-Like Peptide-1 (GLP-1) agonists for childhood obesity and the push in many children’s hospitals to adopt a one-hour fasting interval for clear liquids, contrary to the ASA’s recommendation of two hours. Pulmonary aspiration is a rare complication in children. The APRICOT study, a large, prospective multicenter cohort study of fasted and unfasted children undergoing elective or urgent surgery across 33 European countries in 2017, reported an aspiration incidence of 9.3/10,000, and no cases resulting in severe complications.18
Despite established guidelines, actual preoperative fasting durations in children often exceed recommendations, contributing to increased irritability, nausea, vomiting, dehydration, hypotension, and anxiety.19 Importantly, studies show no significant difference in gastric volume or pH between children who fast for one versus two hours from clear liquids.19 These findings have led several European pediatric anesthesiology societies to endorse a one-hour fasting interval for clear liquids. However, the ASA has maintained its two-hour recommendation, citing insufficient evidence to warrant a change.20
However, fasting guidelines, whether from ASA or international anesthesiology societies, are not absolute standards that can guarantee any outcomes, but solely suggestions to minimize aspiration risk in healthy patients undergoing elective procedures.21 All societies emphasize that the judgement of the anesthesia professional is paramount. Given the limited availability of high-quality, peer-reviewed studies with definitive clinical outcomes on aspiration risk, expert consensus and knowledge of gastric physiology are often the basis for these guidelines.
Considering the low incidence of aspiration with serious outcomes, the difficulty in generating conclusive evidence, and the desire to mitigate the adverse effects of prolonged fasting, gastric ultrasound (especially when paired with image analysis) holds promise as a tool to assess preoperative gastric volume and aspiration risk in children. This approach could support more tailored fasting intervals and facilitate data collection to refine future guidelines, potentially enabling individualized fasting protocols based on real-time assessment.
Processed Electroencephalogram (EEG)
Processed EEG can help improve the precision of anesthetic dosing, as inadvertent overdose is a root cause of many cardiovascular events in unhealthy children, neonates, and infants.22 Moreover, there has been a concern about anesthetics causing neurodevelopmental delay in children, as anesthetics can induce a dose-dependent neuronal degeneration in infant animals. While clinical studies of neurodevelopment in children following anesthesia for surgery have been equivocal, using processed EEG to minimize anesthetic dosing, and over-dose in particular, might lessen this concern. Processed EEG in pediatric anesthesiology remains in early adoption due to lack of devices in many departments, and insufficient research, education, and clinical training with the technology. However, EEG-guided anesthesia education is increasing during residency, fellowships, and society meetings worldwide, and evidence is building.23
Sevoflurane and propofol dosages are based on population studies in healthy children of different ages, which in clinical practice are adjusted to the individual patient based on heart rate, arterial pressure, movement, and for sevoflurane, the expired gas concentration. Thus, current pediatric anesthetic dosages are not based on the brain (hypnosis) or pharmacology studies in unhealthy children.
Until 2018, EEG devices to assess hypnosis emphasized an index number that proved unreliable in young children and those with neurological conditions.23 To have a reliable EEG monitor for hypnosis, the device must display several channels of raw waveform, density spectral array, and index numbers, which are now commercially available.
Pediatric anesthesia professionals using the new EEGs are learning that current dosing practices recommend more sevoflurane and propofol than necessary in all patients, that unhealthy patients often require less dose for the same EEG features as healthy patients, and that inadvertent overdosing is associated with untoward outcomes and safety events.16-18 EEG-guided anesthesia has the potential to transform pediatric anesthesiology practice from “population-based” dosing to “patient-precision” dosing for the brain in all patients.23
Artificial Intelligence (AI)
AI can alert clinicians to high-risk situations before they occur. In pediatric anesthesiology, AI is pre-adoption, and could be added into processed EEG and video laryngoscopy, like image analysis ultrasound. Pediatric anesthesia professionals rely on an EHR that is cumbersome for finding key information, particularly in patients who have complex co-morbidities and who are seen by numerous specialists around the country. AI-integrated EHR could aid in preoperative risk stratification that traditionally has been challenging to predict in children (e.g., airway assessment, blood pressure management, optimization of co-morbidities, transfusion likelihood, and postoperative outcomes and locations). Intraoperatively, AI-assisted monitoring could alert to the potential for adverse events that are critical in the pediatric patient, as well as adjust ventilation settings and medication dosing based on real-time vital signs, weight, and height.17
AI-integrated EHR is also beneficial for pediatric OR management. Workflows and resource allocation can be streamlined, essential for efficiently scheduling the numerous same-day add-on cases more common in pediatrics and the increasing pediatric non-OR case volume.17,24 These technologies can adjust case durations by critical time points in the specific procedure, which would be beneficial for pediatric patients who can have multiple procedures with different specialists under general anesthesia. This will help to reduce cancellations, optimize efficiency, and assist in reduction of costs.17
While AI offers much potential for the workload, it requires large, high-quality datasets, which may not be available for pediatric patients. Barriers include ethical issues when using patient data, especially for vulnerable and small populations, and algorithms are subject to bias and response latency. The high cost, lack of regulations, liability, and implementation requirements can also be barriers in smaller pediatric hospitals.17 Further, there are broad contextual factors considered in clinical judgements by pediatric anesthesia professionals, which may be missed by AI models.
CONCLUSION
Pediatric anesthesiology has evolved dramatically over the past century through successive waves of technological, educational, and organizational innovations that have markedly improved patient safety. As we look to the future, the demands on pediatric anesthesia professionals will intensify with increasing patient complexity and procedural acuity, as the workforce faces shortages. To meet this challenge, the specialty must shift toward proactive system design, resilience, and real-time adaptation of tools to enhance precision and efficiency. Successful adoption will require overcoming barriers related to education, cost, scalability, and trust. By investing in tools within safety science frameworks, pediatric anesthesia professionals can continue to lead in advancing safe, equitable, and high-quality care for the most vulnerable and complex patients.
REFERENCES
- Reich DL. The history of anesthesia and perioperative monitoring. In: Reich DL, Kahn RA, Mittnacht AJC, Leibowitz AB, Stone ME, Eisenkraft JB, eds. Monitoring in Anesthesia and Perioperative Care. Cambridge University Press; 2011:1-8.
- Snow J. On the inhalation of the vapour of ether in surgical operations. J. Churchill; 1847:viii, 88 p. https://www.woodlibrarymuseum.org/rare-book/snow-j-on-the-inhalation-of-the-vapour-of-ether-in-surgical-operations-containing-a-description-of-the-various-stages-of-etherization-and-a-statement-of-the-result-of-nearly-eighty-operations-in-w/ Accessed August 10, 2025.
- Snow J, Richardson BW. On chloroform and other anaesthetics; their action and administration. Br J Anaesth. 1955;27:150–155 PMID: 14351597.
- Kanjia MK, Kurth CD, Hyman D, et al. Perspectives on anesthesia and perioperative patient safety: past, present, and future. Anesthesiology. 2024;141:835–848. PMID: 39377708.
- Gonzalez LP, Pignaton W, Kusano PS, et al. Anesthesia-related mortality in pediatric patients: a systematic review. Clinics (Sao Paulo). 2012;67:381–387. PMID: 22522764.
- Wood-Library Museum History of Anesthesia. American Society of Anesthesiologists. https://www.woodlibrarymuseum.org/history-of-anesthesia/ Accessed May 6, 2025.
- Hache M, Sun LS, Gadi G, et al. Outcomes from Wake Up Safe, the pediatric anesthesia quality improvement initiative. Paediatr Anaesth. 2020;30:1348–1354. PMID: 33078514.
- Warde D. One hundred years ago: The first textbook on anesthesia for children. Paediatr Anaesth. 2023;33:1115–1116. PMID: 37724507.
- Mai CL, Cote CJ. A history of pediatric anesthesia: a tale of pioneers and equipment. Paediatr Anaesth. 2012;22:511–520. PMID: 22443224.
- Stefl ME. To err is human: building a safer health system in 1999. Front Health Serv Manage. 2001;18:1–2. PMID: 11589119.
- Kurth CD, Tyler D, Heitmiller E, et al. National pediatric anesthesia safety quality improvement program in the United States. Anesth Analg. 2014;119:112–121. PMID: 24413551.
- Children’s Surgery Verification. American College of Surgeons. https://www.facs.org/quality-programs/accreditation-and-verification/childrens-surgery-verification/ Accessed May 6, 2025.
- Minehart RD, Stefanski SE. Artificial intelligence supporting anesthesiology clinical decision-making. Anesth Analg. 2025 PMID: 40080433.
- Lingappan K, Neveln N, Arnold JL, et al. Video laryngoscopy versus direct laryngoscopy for tracheal intubation in neonates. Cochrane Database Syst Rev. 2023;5:CD009975. PMID: 37171122.
- Miller AG, Mallory P, Rotta AT. Video laryngoscopy as the standard of care for pediatric intubation-the time is now. Transl Pediatr. 2024;13:537–541. PMID: 38715668.
- Lonsdale H, Eagle SS, Freundlich RE. Machine learning modeling for American Society of Anesthesiologists physical status classification assignment in children. Anesth Analg. 2025;140:e48–e49. PMID: 39883588.
- Lonsdale H, Burns ML, Epstein RH, et al. Strengthening discovery and application of artificial intelligence in anesthesiology: a report from the Anesthesia Research Council. Anesthesiology. 2025;142:599–610. PMID: 40067037.
- Habre W, Disma N, Virag K, et al. Incidence of severe critical events in paediatric anaesthesia (APRICOT): a prospective multicentre observational study in 261 hospitals in Europe. Lancet Respir Med. 2017;5:412–425. PMID: 28363725.
- Thomas M, Morrison C, Newton R, Schindler E. Consensus statement on clear fluids fasting for elective pediatric general anesthesia. Paediatr Anaesth. 2018;28:411–414. PMID: 29700894.
- Joshi GP, Abdelmalak BB, Weigel WA, et al. 2023 American Society of Anesthesiologists practice guidelines for preoperative fasting: carbohydrate-containing clear liquids with or without protein, chewing gum, and pediatric fasting duration—a modular update of the 2017 American Society of Anesthesiologists Practice Guidelines for Preoperative Fasting. Anesthesiology. 2023;138:132–151. PMID: 36629465.
- Practice guidelines for preoperative fasting and the use of pharmacologic agents to reduce the risk of pulmonary aspiration: application to healthy patients undergoing elective procedures: an updated report by the American Society of Anesthesiologists Task Force on preoperative fasting and the use of pharmacologic agents to reduce the risk of pulmonary aspiration. Anesthesiology. 2017;126:376–393. PMID: 28045707.
- Yuan I, Xu T, Skowno J, et al. Isoelectric electroencephalography in infants and toddlers during anesthesia for surgery: an international observational study. Anesthesiology. 2022;137:187-200. PMID: 35503999.
- Kurth CD, Gabrielsen DA, Yuan I. EEG-guided pediatric anesthesia-a quality innovation? JAMA Pediatr. 2025 Apr 21. PMID: 40257772.
- Bellini V, Russo M, Domenichetti T, et al. Artificial intelligence in operating room management. J Med Syst. 2024;48:19. PMID: 38353755.