
Although most of the conversation about the epidemic of prescription opioid abuse centers on chronic pain, opioids also are massively overprescribed for acute pain in children, research shows.
Myron Yaster, MD, professor of anesthesiology at the University of Colorado Denver and an anesthesiologist at Children’s Hospital Colorado, in Aurora, reviewed research showing that opioids are subject to prescription errors at an alarmingly high rate.
Moreover, even when those errors are corrected, opioids are prescribed after surgery in a proportion vastly exceeding actual patient need and are not properly disposed, potentially allowing children and particularly adolescents to get ahold of and abuse these drugs, Dr. Yaster said.
Error Rates: What’s Acceptable?
With regard to prescribing error rates, Dr. Yaster said when he spoke to engineers, they expected that the rate was less than 0.1%, whereas the general public expected the error rate to be under 5%. In sharp contrast, most responders to an audience poll predicted that the error rate exceeds 50%.
“How is that possible? How can we as a business accept a failure rate of 50% or higher?” Dr. Yaster asked. “Would any of you buy a car where you knew that in one out of two cars, the steering wheel was going to fall off? Absolutely not. But we just accept it.”
Dr. Yaster presented the results of a study he participated in at Johns Hopkins Children’s Center, in Baltimore, where he previously worked—and received a lifetime achievement award—that found a discharge prescribing error rate at that institution approaching 80% (J Pain 2009;10:160-166). Following the study, Dr. Yaster and his colleagues instituted an automated prescription-writing program that produced “perfect” prescriptions, he said.
However, he added, that was not the end of the story. Quoting Sherlock Holmes, Dr. Yaster said, “The world is full of obvious things that nobody by any chance ever observes.” He wanted to study prescribing by age, form of medication dispensed and amount of drug dispensed to see whether there were other such “obvious” problems to be found.
One such problem indeed presented itself. In another larger study—in which Dr. Yaster participated—that analyzed nearly 35,000 pediatric outpatient controlled substance prescriptions in the Johns Hopkins database over a seven-year period (Anesth Analg 2016;122:807-813), “regardless of the opioid prescribed, prescribers wrote for very large quantities of opioids,” he said. Nearly half of these prescriptions were written by orthopedic surgeons or their surrogates for acute pain after surgery, he noted.
The study also found that in only 20% of cases were parents given instructions on proper disposal of opioids, but only 4% actually disposed of the drugs properly. That, in turn, resulted in large quantities of opioids—most often kept in kitchen or bathroom cabinets—that can be easily accessed by children and adolescents, who are particularly susceptible to drug abuse, Dr. Yaster said. These findings also were corroborated by a Canadian study (J Pediatr 2015;167:599-604.e1-2).
He added that he himself had leftover oxycodone in a bathroom cabinet from a previous surgery, saying that his aim was not to point fingers but to highlight a widespread problem that needs to be addressed more effectively.
Problem Is Also Acute Pain Control
In the early 1990s, Dr. Yaster said, pain became recognized as a vital sign, prompting a nationwide effort to better treat and manage pain. That change resulted in a rise in opioid prescriptions (Figure 1), which was mirrored by an “astonishing increase in death that absolutely parallels the amount of drug that was dispensed,” he said (Figure 2). Dr. Yaster estimated that the number of deaths was approximately 16,000 per year among adolescents—higher than the number killed by traffic accidents in this age group. He added that adolescents are particularly vulnerable to risky behaviors, and many of them mistakenly believe that prescription opioids are “safer” than street drugs, such as heroin.
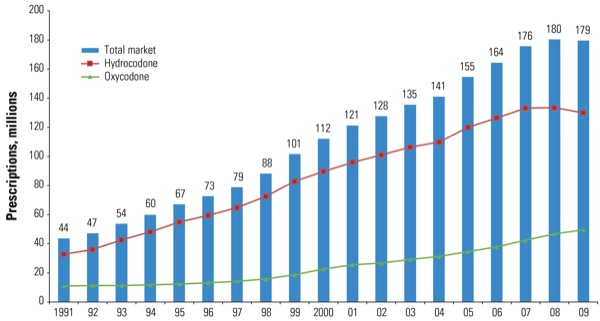
Figure 1. Total number of hydrocodone and oxycodone prescriptions dispensed by U.S. retail pharmacies, 1991-2009.
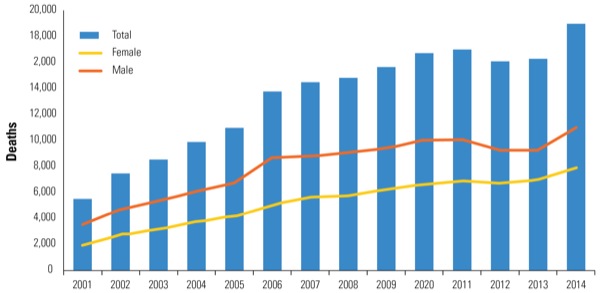
Figure 2. National overdose deaths: number of deaths from prescription opioid pain relievers.
Dr. Yaster’s lecture, which was presented at the 2017 meeting of the Society for Pediatric Anesthesia/American Academy of Pediatrics Section on Anesthesiology and Pain Medicine, concluded with him noting that, while most of the focus of the opioid epidemic has been on chronic pain, acute pain management also plays a role. “We’re also part of this problem, and we’re dispensing much more opioids than these patients need, simply because we have no data to guide prescribers on how much to prescribe. So everybody gets a two- to three-week amount of drugs.”
Lynne Maxwell, MD, FAAP, professor emeritus of anesthesiology and critical care at the Perelman School of Medicine at the University of Pennsylvania, in Philadelphia, and an anesthesiologist at Children’s Hospital of Philadelphia, attended Dr. Yaster’s lecture and agreed with his assessment of the problems described. She noted that she also worked in the same department at Johns Hopkins just prior to the initial study about prescribing errors.
“Now there’s a lot more awareness that the amount and type of drugs that are prescribed post-surgery are not really informed by evidence about how much pain patients experience at home after surgery and how long they need the medication for,” Dr. Maxwell said.
“Regarding the studies that he described, where they developed an automated prescription-writing program, and then they studied how much was actually used by the families at home and how much they used and how much was left of the drug, I think those do represent the type of problem that exists when physicians and other providers write discharge prescriptions for opioids,” she said.
“People end up with a lot of drugs in their houses that aren’t secured and end up going into the reservoir of drugs that’s available for nonprescribed opioid use.”
The bottom line, Dr. Maxwell said, is that anesthesiologists need to take some measure of responsibility for ensuring that patients are safe and comfortable at home after surgery. Having data on how much medicine patients actually need after surgery is a crucial step toward limiting overprescribing, she added.
As an example of the kind of work she would like to see, Dr. Maxwell cited a study conducted by investigators at the Nemours/Alfred I. duPont Hospital for Children, in Wilmington, Del., which examined opioid prescriptions given to children after scoliosis surgery (J Bone Joint Surg Am2016;98:1555-1562). The study found that dosing could be improved by considering patient age, weight, sex and preoperative pain score.
“Raising awareness about this is very important,” she said. “We need to get more information of this type from future studies to inform the prescribers of post-surgery discharge medications, as well as better instructions to families about secure home storage of opioids and safe disposal of unused medication.”