
Abusive behavior in the operating room (OR) is disturbingly prevalent, according to an international study by a team of Canadian clinicians. Given these findings, the investigators called for efforts to eradicate such behavior, including training in violence prevention, de-escalation, stress reduction and anger management.
“Disruptive behavior in the OR implies actions that do not show others an adequate amount of respect, and tends to make victims and witnesses feel threatened,” said Alexander J. Villafranca, MSc, a research associate at the University of Manitoba, in Winnipeg. “This type of behavior is commonplace, and can have detrimental effects on clinicians, students, institutions and even patients.
“A concerning form of disruptive behavior is abusive behavior, which includes both physical abuse, defined as the use of force without consent, and psychological abuse, defined as the use of words or actions to control, frighten or isolate another person.”
Despite the seriousness of such behaviors, few studies have delved into the topic. With that in mind, the researchers sought to estimate the prevalence of exposure to abusive behavior in an international cohort of OR clinicians. Their secondary goal was to identify sociodemographic groups and workplace circumstances that increase the risk for exposure to such behaviors.
Mr. Villafranca and his colleagues distributed surveys via 23 perioperative organizations and four institutions across seven countries. A subsample of respondents from the larger study was also surveyed regarding exposure to three abusive behaviors: physical assault, verbal threats and the invasion of personal space with the intent to intimidate. The researchers used logistic regression to determine predictors of exposure to any of these three behaviors.
“We surveyed anesthesiologists, nurses, surgeons and ‘others’ [technicians and students],” Mr. Villafranca said. “Our survey divided exposure into five categories: exposure to disruptive behavior that was directed toward you, toward colleagues, toward others in the OR, toward patients and undirected behaviors.”
The researchers found that 1,314 of the 2,953 subsample respondents (44.5%; 95% CI, 42.7-46.3) were exposed to at least one abusive event in the preceding year, while 943 (32%; 95% CI, 30.3-33.7) were exposed to multiple abusive events (Figure).
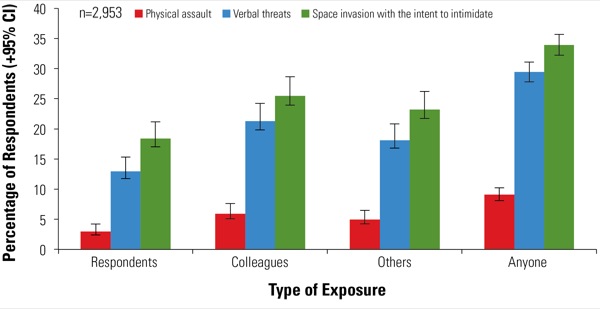
Specifically, 34% of respondents were exposed to someone having their personal space invaded, 29% were exposed to someone being verbally threatened, and 9% were exposed to someone being physically assaulted. “Bear in mind that this is in the preceding 12 months, not lifetime exposure,” Mr. Villafranca said.
He and his colleagues then analyzed individual exposure to such events. “We did this because it was impossible to determine if witnessed behaviors included the same event being reported by multiple people,” he said. “And when we looked at this, the numbers were staggering.”
Indeed, more than 1,000 assaults were reported by 85 respondents, more than 5,000 verbal threats were reported by 372 respondents, and nearly 10,000 personal space invasions with the intent to intimidate were reported by 528 people. In total, more than 16,000 abusive events were reported by 699 clinicians.
“We can argue all day about response rates and the prevalence estimates, but the bottom line is that when a group of clinicians is telling you that they’ve personally experienced thousands and thousands of abusive events in a single year, we need to take their words seriously and look into this issue more.”
Respondents more likely to report exposure to abuse included nurses, individuals with nonheterosexual orientations and those in management positions (all P<0.05). Of note, exposure to less egregious disruptive behavior was predictive of exposure to abusive behavior (all P<0.001), unless the disruptive behavior was directed either toward patients (P=0.07) or no one in particular (P=0.08).
“This potentially indicates that if you survey your environment for those three forms of less egregious behaviors, it may give you some indication as to whether abuse exists in your operating rooms,” Mr. Villafranca said.
Although documenting the prevalence of the problem is an important piece of the puzzle, the most important step is addressing it. “So what do we do about this problem?” Mr. Villafranca asked. “It’s clear that we need to make further efforts to get the frequency and prevalence down to zero; these should be never events.
“This is a complex social problem, and there aren’t easy solutions,” he continued. “So preliminary useful steps in eliminating abusive behavior would be to provide clinicians with soft skills training in violence prevention, de-escalation techniques, stress management and anger management.”
“Did you see many regional variations around the world or did you find it to be equally distributed?” asked one of Mr. Villafranca’s audience members.
“There are definitely differences between countries,” he replied. “But I really wanted to stay away from documenting those differences, because when you’re looking at the issue in other countries, there’s sometimes a reluctance. So we had certain institutions that agreed to help us, and I didn’t want to point the dirty end of the stick at those institutions.”
Karen L. Posner, PhD, the Laura Cheney Professor in Anesthesia Patient Safety at the University of Washington, in Seattle, raised a question about the survey’s methodology. “Were your subjects given those definitions of abuse when they answered the survey?”
“No,” Mr. Villafranca answered. “Here’s the thing: When you ask patients if they’ve been exposed to certain abusive behaviors, you get one prevalence estimate. But if you ask if they’ve been a victim of abuse, you get a prevalence estimate that is about 25% of that. So people are very hesitant to self-label. The better way to approach things is to ask people if they’ve been exposed to certain behaviors.”