
Authors: Yvon F. Bryan, MD and Kathleen N. Johnson, BS
Introduction
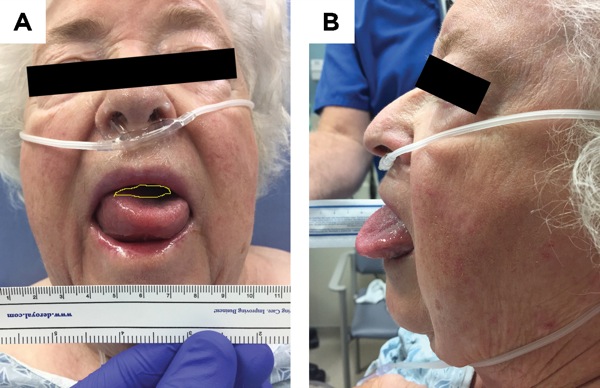
Angioedema is a rare condition that results in localized swelling of subcutaneous or submucosal tissue in the oral cavity.1,2 Patients suffering from angioedema may require airway management depending on the degrees of severity and swelling.3 There are different airway management strategies to treat this condition, from noninterventional to a surgical airway.4 Assessing the airway and degree of airway compromise is critical in deciding a definitive treatment. Obtaining serial photographs in order to measure the amount of unoccupied area in the oral cavity using digital imaging is an effective way to guide that decision-making process.5,6
If the swelling is minor, then the condition may be initially treated medically with the administration of antihistamines, steroids and/or epinephrine.7 If treated medically, it is still imperative to monitor the regression of swelling in the manner described above.6 However, if the case is severe, then there may not be time to evaluate with digital imaging, as the intervention to secure the airway may be urgent. With the time constraints placed depending on the severity, deciding on the best airway management technique is key, as changes to the intended plan may result in complications. A specialized airway device, such as a flexible fiber-optic bronchoscope (FFB), offers finesse and maneuverability in the oral or nasal cavity. This is beneficial due to the severe swelling, which limits the space of the oral cavity that is not occupied by the tongue. Additionally, as the case is oftentimes emergent and the patient is likely not “nothing by mouth” status, reducing the risk for aspiration by awake intubation is imperative.
Furthermore, management of these patients is more challenging in rural care settings.8 Less resources are available in the emergency department (ED) in these settings, and the patient may require transfer to the OR for management. With the lack of an ICU, transfer after definitive care to a tertiary care center may be required. Additionally, in an urgent case it is important to be able to obtain the necessary equipment, local anesthetics for topicalization, etc., in a timely fashion, which may be more difficult in small community hospitals. We present a case of severe angioedema in a small community hospital and the implications it has on emergent airway management in rural settings.
An 86-year-old woman with a body mass index of 26.2 kg/m2 and a history of hypertension presented to the ED of a small community hospital at 1:45 a.m. with severe swelling of the tongue and oral cavity. Anesthesia was consulted for airway management. Upon arrival and evaluation by a physician in the ED, the anesthesiologist assessed the airway and consulted general surgery for backup in case a surgical airway was required. The patient had been treated with methylprednisolone, diphenhydramine and famotidine in the ED. The decision was made to transport the patient to the OR for awake nasal intubation with an FFB and minimal sedation (1 mg of IV midazolam and 25 mcg of IV fentanyl) (Figure 1A-O).










Overview of Technique
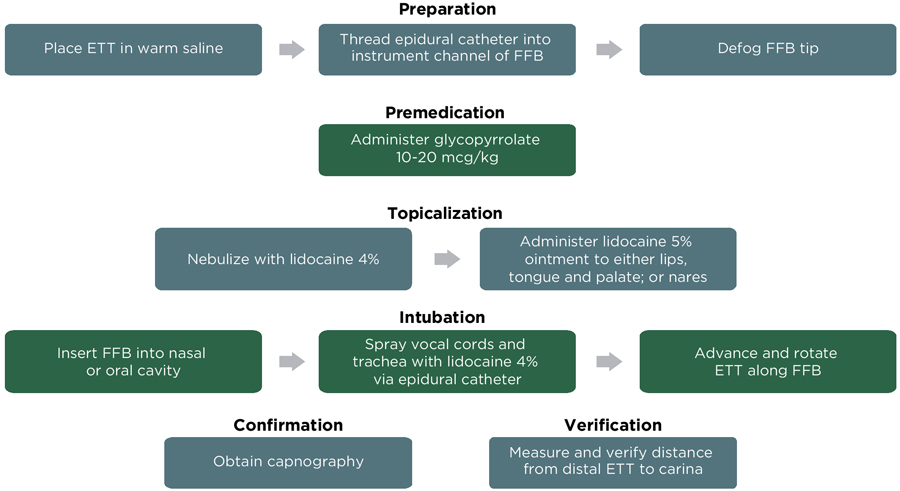
Preparation
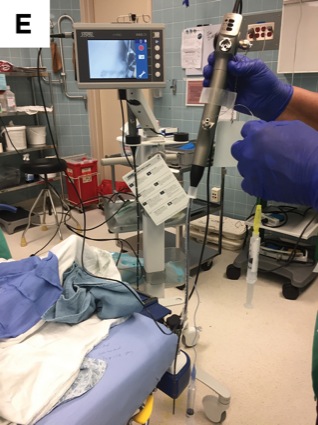
Consider placing a smaller diameter endotracheal tube (ETT) in warm saline water, and wrap it with a warm blanket to soften the tube. Similarly, obtain a small-diameter FFB and defog it to ensure adequate visualization. Thread an epidural catheter through the instrument channel of the FFB in order to administer local anesthetic to the glottis.
Premedication
Premedicate with an antisialagogue to reduce secretions. It is also important to suction the oral and nasal cavities. Minimal sedation should be used to decrease the likelihood of complications related to oxygenation.
Topicalization
For nasal intubation, administer lidocaine 5% ointment to the nares. For oral intubation, administer to the tongue, palate and oral cavity using a tongue dispenser and intubating oral airway.
Intubation
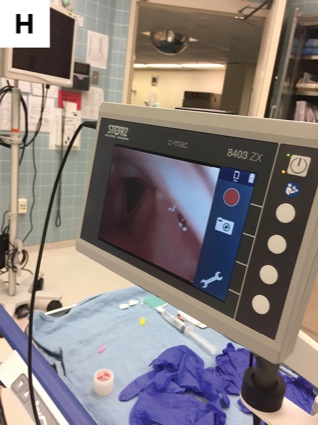
Insert the FFB, taking caution to avoid the edematous areas to avoid secretions and minimize bleeding. Once a view of the glottis is obtained, the lower airway should be topicalized with lidocaine 4% sprayed through the epidural catheter that was threaded in the instrument channel. The ETT may then be advanced using a clockwise–counterclockwise rotation (Figure 2).
Conclusion
As previously stated, time is of the essence in cases such as the one described. It is important to be able to easily and more efficiently obtain the resources required for airway management, especially in a rural hospital. We developed a checklist to have on hand in these cases to ensure the best possible preparedness, especially if the patient arrives in the middle of the night (Figure 3).



Ointments (A)
- 2 lidocaine 4% 5-mL vials (not shown)
- Nebulizer (not shown)
- Lidocaine 5% ointment
- Lidocaine 2% jelly (backup)
- Lubricating jelly
- Tongue depressor
- Gauze
Airways (A)
- Oral airway
- Ovassapian airway
- 28, 30, 34 Fr nasopharyngeal airways
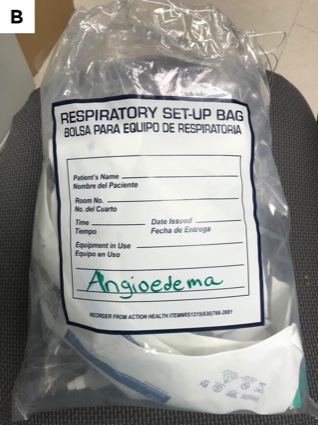
Oxygen and Suction (B)
- Nasal cannula
- 10 Fr
- 14 Fr
- 18 Fr
- Yankauer (not shown)
Endotracheal Tubes (C)
- For oral/nasal use (0.5- to 1.0-mm smaller ID)
- 10-mL syringe
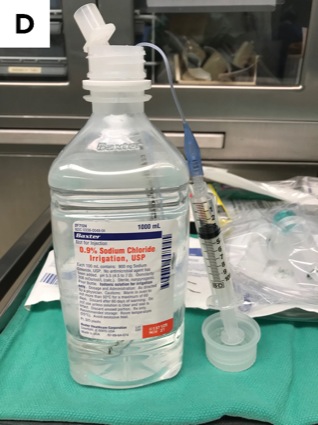
- Warm saline bottle to wrap in warm towel
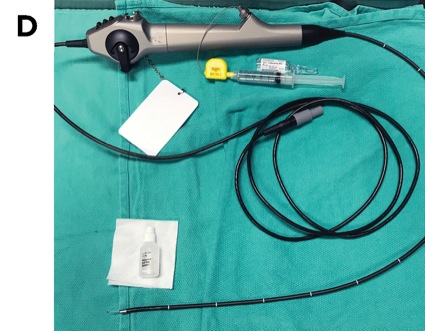
- Fiber-Optic Bronchoscope (D)
- FFB
- Defogger
- Epidural catheter with 5-mL syringe for lidocaine 4%
In addition, we have found that having the resources on hand is most important in improving management in a small hospital to reduce the amount of time spent gathering supplies and going to the pharmacy, which may not be open late at night. For this reason, we have an angioedema kit in which all of the necessary resources are stored in a bag that may easily be accessed in case of emergent airway management (Figure 4).

Ultimately, preparedness and proper evaluation of the patient are imperative for the management of angioedema. This may be done safely in a small community hospital if the necessary steps are done to minimize time and maximize the available resources.
References
- Zuraw B, Bingham CO III. An overview of angioedema: clinical features, diagnosis, and management. In: Feldweg AM, ed. Waltham, MA: UpToDate; 2016.
- Moellman JJ, Bernstein JA, Lindsell C. A consensus parameter for the evaluation management of angioedema in the emergency department. Acad Emerg Med. 2014;21(4):469-484.
- Ishoo E, Shah UK, Grillone GA, et al. Predicting airway risk in angioedema: staging system based on presentation. Otolaryngol Head Neck Surg. 1999;121(3):263-268.
- Chiu AG, Newkirk KA, Davidson BJ, et al. Angiotensin-converting enzyme inhibitor-induced angioedema: a multicenter review and an algorithm for airway management. Ann Otol Rhinol Laryngol. 2001;110(9):834-840.
- Bryan YF, Johnson KN, Riley Z, et al. The use of digital imaging to measure the tongue and unoccupied area in the oral cavity: an alternative technique for precise objective airway assessment. Anaesth Pain Intensive Care. 2018;22(3):301-307.
- Bryan YF, Johnson KN. The difficult airway in adults with angioedema. Anesthesiology News Airway Management. 2018;suppl:95-98.
- Chan NJ, Soliman AM. Angiotensin converting enzyme inhibitor-related angioedema: onset, presentation, and management. Ann Otol Rhinol Laryngol. 2015;124(2):89-96.
- Bryan YF, McLaughlin DH, Johnson KN, et al. The use of flexible fiberoptic bronchoscopy for nasal intubation in a patient with severe angioedema of the oral cavity in the emergency room; neither conventional laryngoscopy by ED nor tracheostomy by ENT but FFB by anesthesiology. Anesthesiology. 2017;MC2043.
Leave a Reply
You must be logged in to post a comment.