
Author: Michael Vlessides
Anesthesiology News
A meta-analysis of adjuvants for caudal epidural block has found that dexmedetomidine prolongs the duration of analgesia and also reduces total acetaminophen consumption and number of acetaminophen doses in the first 24 hours after pediatric infraumbilical surgery.
The study also found that neostigmine extended the analgesia duration longer than any of the other adjuvants studied.
“In recent guidelines, the European and American societies of regional anesthesiologists recently recommended the use of caudal blocks for various infraumbilical procedures,” said Niveditha Karuppiah, MD, a clinical fellow in anesthesia at the University of Western Ontario’s London Health Science Center, in London. “They also go on to suggest the use of adjuvants to prolong the duration of the caudal block.
Ranking Adjuvant Efficacy
Although several adjuvant medications have been shown to extend analgesia in these blocks, the relative efficacy of these drugs—clonidine, dexamethasone, dexmedetomidine, fentanyl, ketamine, magnesium, morphine, neostigmine and tramadol—is still unknown. The investigators therefore conducted a meta-analysis of randomized controlled trials (RCTs) to help synthesize and rank the adjuvants’ comparative effectiveness in pediatric infraumbilical surgeries.
“The population included pediatric patients undergoing infraumbilical surgeries with or without general anesthesia and receiving a caudal block,” Dr. Karuppiah said. The intervention arm consisted of patients given a caudal block with a long-acting local anesthetic and any caudal adjuvant in any dose. The control group had a caudal block with only a long-acting local anesthetic, which was bupivacaine or ropivacaine.
In presenting the study at the 2019 annual meeting of the Canadian Anesthesiologists’ Society (abstract 637521), Dr. Karuppiah noted that 671 articles were screened and 70 were included in the analysis.
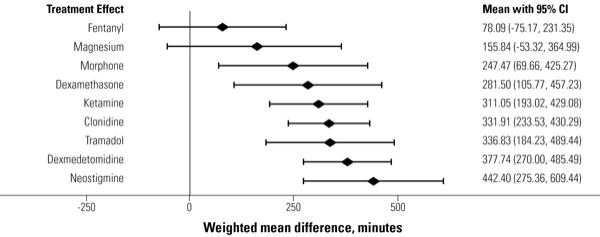
Mixed-evidence synthesis from these 70 trials, involving 4,258 patients, indicated that neostigmine prolonged analgesia duration by 442.40 minutes (95% CI, 275.36-609.44 minutes), followed by dexmedetomidine (377.74 minutes; 95% CI, 270.00-485.49 minutes). Neither caudal fentanyl nor magnesium was superior to the control anesthetic (Figure).
With data on the total 24-hour postoperative acetaminophen dose from 23 RCTs including 1,448 patients, only dexmedetomidine was found to be superior to control (–1,470.62 mg; 95% CI, –2376.86 to –564.37 mg). Dexmedetomidine was ranked the best of the adjuvants for this outcome (Table).
| Table. Analgesic Outcomes by Adjuvant Use | ||||||
| Analgesia Duration, minutes | Total Acetaminophen Doses, mg | Acetaminophen Doses, n | ||||
|---|---|---|---|---|---|---|
| WMD | Rank | WMD | Rank | WMD | Rank | |
| Neostigmine | 442.4 | 1 | –118.48 | 7 | –0.54 | 5 |
| Dexmedetomidine | 377.74 | 2 | –1470.62 | 1 | –1.31 | 1 |
| Tramadol | 336.83 | 3 | –138.77 | 6 | –0.89 | 4 |
| Clonidine | 331.91 | 4 | –144.38 | 5 | –0.93 | 3 |
| Ketamine | 311.05 | 5 | –184.41 | 4 | –1.20 | 2 |
| Dexamethasone | 281.50 | 6 | –103.02 | 8 | –0.33 | 7 |
| Morphine | 247.47 | 7 | –1067.92 | 2 | NA | – |
| Magnesium | 155.84 | 8 | NA | – | –0.47 | 6 |
| Fentanyl | 78.09 | 9 | –864.85 | 3 | NA | – |
| NA, not available; WMD, weighted mean difference | ||||||
In 13 RCTs with 883 patients, the number of 24-hour acetaminophen doses also was reduced most by dexmedetomidine (–1.31; 95% CI, –1.72 to –0.90).
According to Dr. Karuppiah, the overall risk for bias was found to be low in 27 of the RCTs, although there were some concerns noted in 45 trials, and one trial showed a high risk for bias. All outcomes had a “moderate” level of evidence.
“Dexmedetomidine was the only one that showed a benefit across all the primary and secondary outcomes,” Dr. Karuppiah said. “Contrary to popular belief, both morphine and fentanyl—the opioids we tend to use—did not fare that well.
“This review hopefully helps clinicians decide which adjuvant would work best and know the order in which they could be used,” Dr. Karuppiah said. “It also adds to the existing literature, and it will hopefully guide future studies with respect to safety outcomes.”
“I’m curious how you dealt with heterogeneity within the studies, things like the ages of the patients; the volume and concentration of local anesthetic; and the use of IV versus perineural adjuvants, such as concomitant dexamethasone,” said Thomas Mutter, MD, an assistant professor of anesthesia at the University of Manitoba Faculty of Medicine, in Winnipeg.
“For the sake of this abstract and presentation, we haven’t done the subgroup analyses or specifically examined heterogeneity,” Dr. Karuppiah replied. “But I can tell you the heterogeneity is on the higher side. We’ll have to analyze it further to see what effect it has on the results.”
Leave a Reply
You must be logged in to post a comment.