
Anesthesiology practitioners in a multispecialty setting used a deep neuromuscular block (NMB) on average 64% of the time, according to a retrospective study.
“The goal was to understand what clinicians do in real clinical practice,” said co-author Richard D. Urman, MD, associate professor of anesthesia at Brigham and Women’s Hospital, in Boston. “We examined the entire spectrum of surgical procedures.”
Dr. Urman noted that there is already plenty of evidence regarding adverse events from residual NMB, including residual paralysis, respiratory complications and the need for reintubation.
The expected duration of the case was calculated based on the cumulative dose of NMB used, normalized to the patient’s ideal body weight and the ED95 (effective dose, 95%) of the drug. If the expected duration of the case was greater than the actual case duration documented in the case record, it was classified as deep NMB. Conversely, if the expected duration was equal to or less than the actual duration, it was considered moderate NMB.
Categorical comparisons between deep and moderate NMB groups were made for variouspatient, procedural and provider factors.
“For the study, we actually did not use train-of-four (TOF) monitoring as an estimate,” said Dr. Urman of the Merck-funded study. “Being a retrospective study, we do not know when clinicians measured TOF versus when they documented it.” In addition, not all cases had a documented TOF.
The use of NMB was stratified by patient factors (morbidly obese vs. normal body mass index; elderly vs. nonelderly) and procedure factors (laparoscopic vs. open; rapid sequence intubation [RSI] vs. non-RSI; total IV anesthesia [TIVA] vs. volatile anesthesia; and emergent vs. nonemergent cases).
Various large and small surgeries were also taken into account. “Minimally invasive surgery, mostly laparoscopic surgery, was more likely to have a deeper NMB, which we suspected,” Dr. Urman said (Figure).
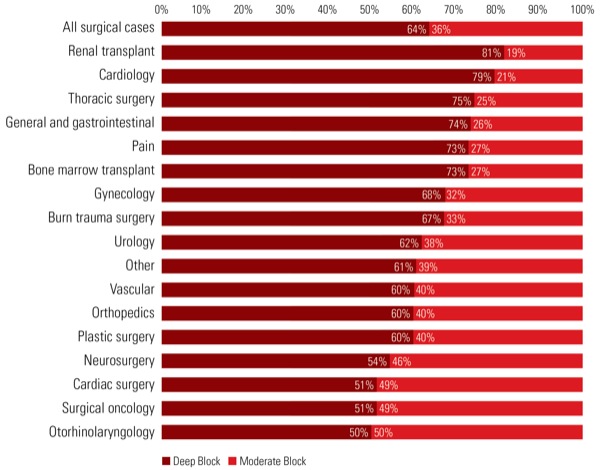
Renal transplant cases had the highest proportion of deep NMB (81%), whereas orthopedic (60%), neurosurgical (54%), cardiac (51%) and otorhinolaryngology (50%) cases had some of the lowest proportions (Figure).
Other factors associated with deep NMB were morbid obesity (70%), emergent cases (69%), TIVA (68%) and cases that did not involve RSI (64%).
However, patients older than 65 years had a lower rate of deep NMB (60%) compared with younger patients (65%). “This was likely due to age-related changes in pharmacokinetics, resulting in a more significant paralytic effect at the same dose, and thus less of an agent was needed for the case,” Dr. Urman said. “It may also reflect anesthesia provider practices.”
Identifying the Need for Reversal Agents
On the other hand, a reversal agent such as neostigmine was used in 85% of deep NMB cases as opposed to 71% of moderate NMB cases. “This finding reflects provider awareness of a deeper block,” Dr. Urman said.
The time span of the retrospective study was before the reversal agent sugammadex (Bridion, Merck) became available at Brigham and Women’s Hospital.
“Although our study only looked at the rates of moderate versus deep paralysis, our results can be used to help recognize factors associated with deep NMB in order to identify patients at higher risk for residual paralysis and to increase monitoring intra- and postoperatively,” Dr. Urman said.
The study authors would like to use their findings to create pharmacoeconomic models to understand the benefits of novel reversal agents.
Stephan Thilen, MD, associate professor of anesthesiology and pain medicine at the University of Washington, in Seattle, is not surprised by any of the study results. “However, a major limitation is the definition of deep block,” he said. “The conventional definition of deep block is a block with a TOF count of [zero]. In this study, it is not known whether deep block was actually present.”
Dr. Thilen said, “We need to stop overdosing our patients with neuromuscular blocking drugs. Overdosing often starts with intubation; for example, 50 mg of rocuronium is not required for intubation in the majority of patients.”
Dr. Thilen also said deep NMB should be used only when indicated. “Indications for deep block are not present in the vast majority of cases in a mixed surgical population.”
In addition, reversal should always begin with a valid pre-reversal assessment at the adductor pollicis, according to Dr. Thilen. “Without knowing the exact depth of the block, it is not possible to consistently conduct a successful reversal in each case,” he said.
In the future, quantitative monitoring “will no doubt become routine,” Dr. Thilen said. “But we also need deeper insights into how much paralysis is actually required and a better appreciation for the substantial interpatient variation that exists in the response to muscle relaxants.”
Improved communication in the operating room between anesthesiologists and surgeons over the requirement for paralysis also is key. “Sometimes paralysis is not required through the end of surgery, allowing for more spontaneous recovery and a shallower block at the conclusion of the procedure,” Dr. Thilen said.
Leave a Reply
You must be logged in to post a comment.