
The Doctor’s Advocate | Fourth Quarter 2019
Anesthesiologists have taken a leading role in efforts to reduce the risk of harm to patients. Pulse oximetry was introduced in the late 1970s, followed by numerical end-tidal CO2 monitoring in the 1980s. The Anesthesia Patient Safety Foundation was founded in 1985 with the stated mission of working toward the time when “no patient will be harmed by anesthesia care.”
Significant improvements to care include graphical display of capnography, ultrasound-guided regional anesthesia and central line placement, transesophageal echocardiogram monitoring, screening for obstructive sleep apnea (OSA), and introduction of airway classifications. These improvements and practice guidelines have made administration, management, and monitoring of anesthesia care safer.
We have been studying anesthesia claims since 2007. While most physician specialties have seen double-digit decreases in rates of claims in the last 12 years, claims filed against anesthesiologists have decreased from 6 percent (per 100 full-time equivalent practitioners) in 2006 to around 4 percent in 2018. Although the rates of anesthesiology claims are low, this study may indicate limited movement toward further improvement.
Our first study of anesthesia claims, which included claims from 2007 through 2012, was published in the Journal for Healthcare Risk Management in 2013. In June 2019, we repeated the study for claims that closed between 2013 and 2018, with claims for pain medicine and tooth damage excluded. The second study, which reviewed 459 claims for patient injuries, analyzed new trends in claims involving anesthesia care.
Our recent study showed that the two most common anesthesia allegations—improper management of patients under anesthesia (32 percent) and improper performance of anesthesia procedures (27 percent)—had not changed from the previous study. However, the order of frequency was reversed. In the 2007 through 2012 study, improper management of patients under anesthesia represented 22 percent of allegations, and improper performance of anesthesia procedures represented 34 percent. (See FIGURE 1.)

Improper Management of Patients Under Anesthesia Allegations
Analysis of improper management of patients under anesthesia revealed that the most common reason for the alleged mismanagement was selection and management of therapy. In most cases, the allegation referred to management of complications that occurred during surgery. We noted that 55 percent of these cases had respiratory complications, central nervous system complications, adverse effects of anesthesia, or cardiac complications.
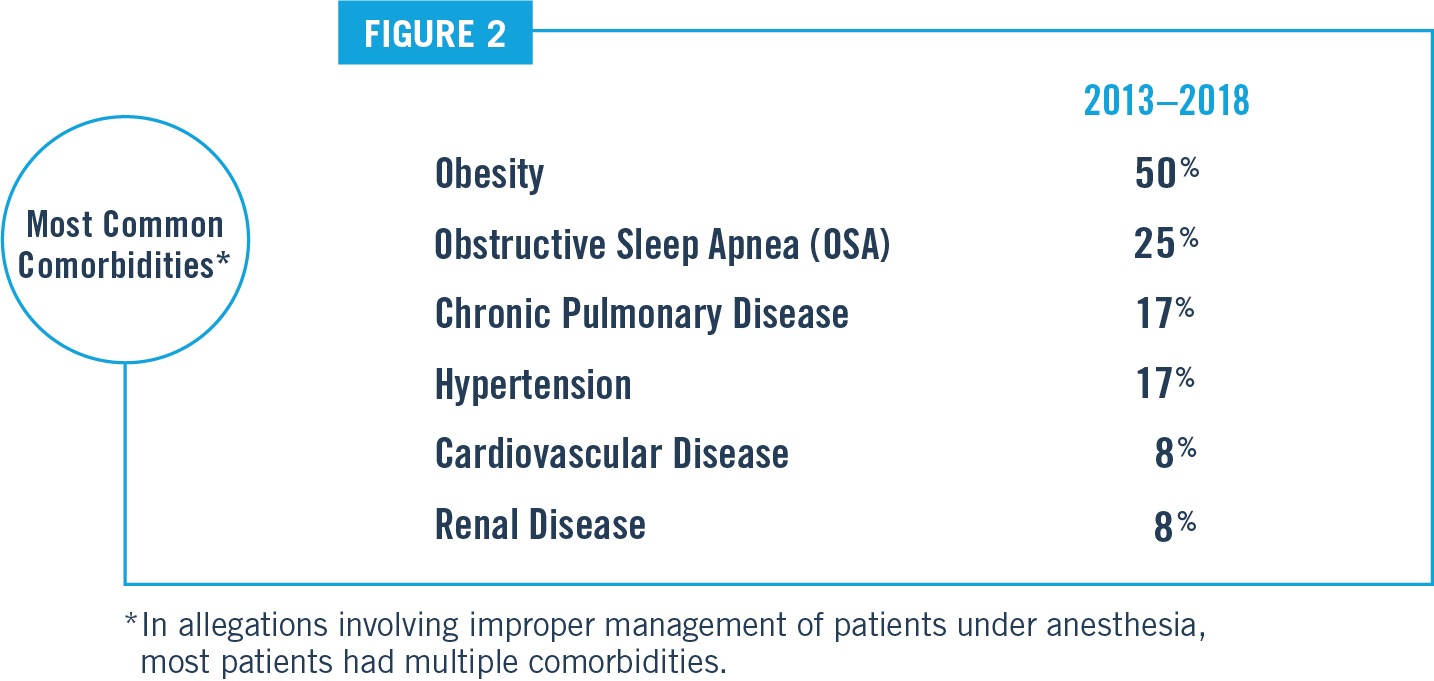
A deeper review of these cases revealed that when physician reviewers identified inadequate histories and physicals, 67 percent of patients had at least one comorbidity (patients averaged 2.2 comorbidities) that affected the outcome of care. The most common comorbidities were obesity (50 percent), OSA (25 percent), chronic pulmonary disease (17 percent) hypertension (17 percent), cardiovascular disease (8 percent), and renal disease (8 percent). (See FIGURE 2.)
These findings, plus the factors contributing to patient harm that physician reviewers identified, provide insights into deficiencies. The top three factors identified in claims were deficiencies in patient assessments (including histories and physicals), patient monitoring, and communication among providers.
A review of cases revealed limited opportunities to conduct pre-op assessments. Older and sicker patients needed closer investigation, but production pressures often limited testing and input from attending or referral physicians. These pressures also limited anesthesia professionals’ opportunities to arrange for the safest location for anesthesia care (hospital operating room versus a remote ambulatory surgery center or GI or cardiac labs) or to prepare for complications that might occur as a result of multiple comorbidities or complicated health histories.
Case Study: Selection and Management of Therapy
A 48-year-old obese (BMI 38.6) male saw an orthopedist due to a work-related torn meniscus. The patient was sent to an internist for “clearance” before anesthesia and surgery, and a pre-surgical EKG was completed.
The internist noted the patient had hypertension, diabetes mellitus, hypercholesterolemia, and a history that his parents had died in their 60s of suspected coronary artery disease. The patient’s blood pressure was elevated. He had severe and untreated OSA. His medications—including metformin, glipizide, lisinopril, metoprolol, and amlodipine—were started, and follow-up showed better control of hypertension. The patient was medically “cleared” for surgery.
The anesthesiologist rated the patient as ASA III with an airway Mallampati score of three. The patient underwent left knee arthroscopy in an ambulatory surgical center. An anesthesiologist provided sedation consisting of 100 mcg of fentanyl and 2 mg of Versed before inducing general anesthesia with propofol. A laryngeal mask airway (LMA) was placed, and general anesthesia was maintained with 3 percent inhaled sevoflurane. End-tidal CO2 was recorded as 8 percent (about 60 torr) with a spontaneous respiratory rate (RR) of eight breaths per minute. Surgery to repair a torn meniscus proceeded without complication.
The LMA was removed in the OR with no sign of aspiration. On arrival in the PACU, the patient had the following vital signs: BP 184/98, HR 92, RR 20, oxygen saturation 84 percent. He required nursing to provide jaw thrust and insertion of nasal and oral airways. He was unresponsive for about 20 minutes. The patient eventually awakened from anesthesia but remained sleepy. He was more arousable after Narcan 40 mg. The orthopedist left the facility. The patient seemed awake, alert, and conversing, but he still had decreased oxygen saturations.
The anesthesiologist noted pulmonary crackles, and the patient was encouraged to take deep breaths and cough. The patient complained of shortness of breath. His RR increased to 30 BPM. Lasix 40 mg was given 45 minutes after arrival in the PACU without marked improvement. A second dose of Lasix was given 30 minutes later. The anesthesiologist ordered an EKG, which showed no changes compared to the pre-op EKG. After another 30 minutes, an albuterol nebulizer x 1 was administered with better air movement, but bradycardia was down to the 40s. The patient’s oxygen saturations remained in the 80s, with a single recorded saturation of 95. The plan was to intubate him prior to further respiratory failure and to transfer him to an ER for more evaluation.
Two hours after arrival in the PACU, the anesthesiologist applied an Ambu bag and assisted ventilation. The patient was easily intubated on one attempt. Copious pink frothy fluid was noted on placement of the endotracheal tube. The tube was suctioned. The orthopedist was informed and met them in the ER.
The anesthesiologist stayed with the patient as he was transported to the hospital by ambulance. During transit, bradycardia down to the 40s was noted. Oxygen saturation remained in the 80 percent range.
Shortly after arriving in the ER, the patient went into asystolic arrest. The ER physician made five attempts to place transvenous pacing but could not pass the wire. CPR continued for over 30 minutes before the patient was pronounced dead.
At some point, a nasogastric tube returned 400 ml of coffee grounds‒colored emesis. This was most likely the result of swallowing bloody pulmonary edema fluid.
The autopsy noted no apparent airway obstruction. The pathologist determined that the cause of death was flash pulmonary edema. Negative pressure pulmonary edema (NPPE) is a cause of rapid onset, or flash, pulmonary edema. NPPE is caused by vigorous inspiratory efforts against an obstructed upper airway, a complication that can occur during sleep or somnolence after general anesthesia.
Some experts who reviewed this case opined that the LMA had been removed too soon because of OSA and the Mallampati score of three. They also stated that intubation was delayed, especially considering the previously elevated end-tidal CO2. If end-tidal CO2 measurements or arterial blood gases had been available in the PACU, it is possible that the time course of therapy might have been expedited. In considering the patient’s comorbidities, some questioned performing the procedure in an outpatient setting. It is unknown whether production pressure before and after the OR anesthesia care may have contributed to the eventual poor outcome in this case.
Improper Performance of Anesthesia Procedures Allegations
In our study, improper performance of anesthesia procedures was the second most common allegation, accounting for 27 percent of the claims. The most common factor that contributed to patient injury was technical performance (88 percent).
The improper performance of anesthesia procedures arose from intubation of the respiratory tract, injection of anesthesia into a peripheral nerve, and injection of anesthesia into the spinal canal. Intubation cases resulted from injuries during intubation or from improperly located endotracheal tubes, causing hypoxia. Injection of anesthesia into the spinal canal cases occurred when the injection was incorrectly placed as spinal (not epidural) anesthesia.
Injection of anesthesia into a peripheral nerve or peripheral nerve blocks sometimes resulted in nerve damage or inadvertent injection into or near blood vessels. The frequency of these cases has been decreasing in recent years due to the use of ultrasound-guided needle placement. As with all cases, lack of documentation or inadequate documentation (18 percent) may impact the quality of care and the anesthesiologist’s ability to defend the care provided.
Risk Mitigation Strategies
The following strategies can assist physicians and providers in reducing risk and improving quality of care:
- Include information in the informed consent about anesthesia risks, including special positioning risks and risks of special procedures like nerve blocks and arterial lines. Patients with dental conditions or teeth at risk need to be specifically informed.
- Work with your surgeons, proceduralists, and healthcare organizations to ensure adequate time for preoperative assessments and testing. Some anesthesiologists report pressure to proceed with surgery when they have not had time to do more than a cursory review of the patient and his or her history.
- Include a review of the patient’s previous experience with anesthesia in the history and physical. If possible, review previous anesthesia records.
- Tailor an anesthesia plan for each patient to specifically address any abnormal findings from the history or physical exam.
- Fully document the preoperative anesthesia assessment. In the case discussed in this article, the presence of severe untreated OSA should have dictated a late removal of the LMA only after the patient was fully awake.
- Rely on your examination of the patient’s signs during anesthesia care rather than assuming that OR equipment is defective when it appears to be malfunctioning. Relying on or ignoring monitors rather than examining the patient is one of the most frequent cognitive errors made by anesthesia providers.
- Communicate concerns about the patient’s physiological condition to the OR team. Most anesthesia providers are reluctant to speak up about the patient’s condition unless they detect severe or pre-arrest symptoms.
- Ensure that equipment and supplies for emergency tracheostomies are immediately available in the postanesthesia area.
- Monitor the mean arterial pressure in cases that involve bleeding and positioning to prevent brain injury from inadequate oxygenation during surgery. More importantly, do not assume that a mean pressure of the traditionally taught 60 torr is adequate for cerebral circulation for all patients and for all surgical positions.