
Since 2009, Anaesthesia has published annual special issues focusing on novel and clinically-important topics in peri-operative medicine, critical care and pain. This year, for the first time, we are revisiting a subject that was previously featured in 2009: regional anaesthesia. This is an acknowledgement, not only of widespread public interest, but also the fundamental importance of this field in modern anaesthetic practice, and the pace of innovation in recent years.
The accompanying editorial highlights what we believe is the next frontier: increasing patient access to safe and effective regional anaesthesia. The evolution of regional anaesthesia is marked by multiple pivotal innovations that have driven its rise in popularity within our specialty (Fig. 1). These have transformed it from an arcane art practiced only by enthusiasts to a core skillset taught to all trainees. This, however, has also been accompanied by an increased complexity in scope that threatens to overwhelm the general practitioner. There is thus a need to refine, and even simplify, our techniques to maximise provider uptake and in turn, patient benefit.
Four key themes run through the supplement: safety, efficacy, quality and innovation.
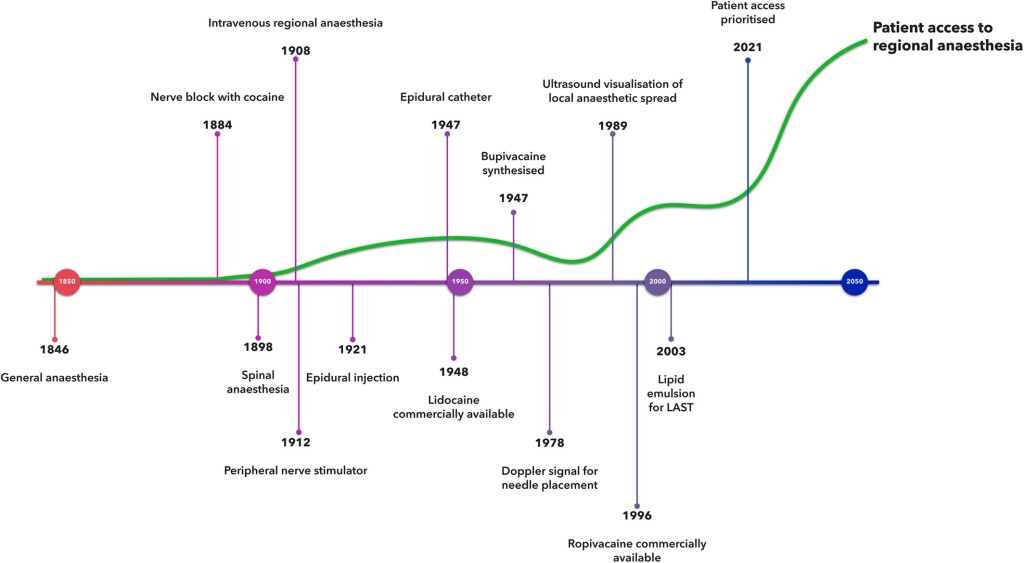 Figure 1. Key landmarks in the development of regional anaesthesia along with changes in patient access to regional anaesthesia over time (green line). LAST, local anaesthetic systemic toxicity. From Chin, Mariano and El-Boghdadly (2021).Safety
Figure 1. Key landmarks in the development of regional anaesthesia along with changes in patient access to regional anaesthesia over time (green line). LAST, local anaesthetic systemic toxicity. From Chin, Mariano and El-Boghdadly (2021).Safety
Nerve localisation has traditionally been based on landmark or peripheral nerve stimulator-guided techniques. Not surprisingly, this has declined in recent years with the advent of ultrasound-guided approaches. However, rather than abandoning the use of nerve stimulation entirely, Dr Gadsden recommends that we reframe its purpose. Instead of using it to tell us when we are ‘close enough’ (a tool for efficacy), we should use it in combination with ultrasound visualisation of the needle tip to tell us when we are ‘too close’ (a tool for safety). As he states in a clever analogy, why choose between seatbelts or airbags when you can have both?
Macfarlane et al. delve further into the safety of regional anaesthesia, providing an up-to-date understanding of local anaesthetic systemic toxicity (LAST). This is still a highly-relevant complication even in the era of ultrasound-guidance, and there have been important changes in the typical clinical presentation thanks to the current enthusiasm for fascial plane blocks, intravenous lidocaine infusions and high-dose local anaesthetic infiltration techniques by non-anaesthetists. The authors highlight the considerations pertinent to modern anaesthetic practice and also describe a management algorithm that incorporates technique- and patient-related risk factors (Fig. 2). We would consider this paper essential reading for any clinician using local anaesthetics in their practice.
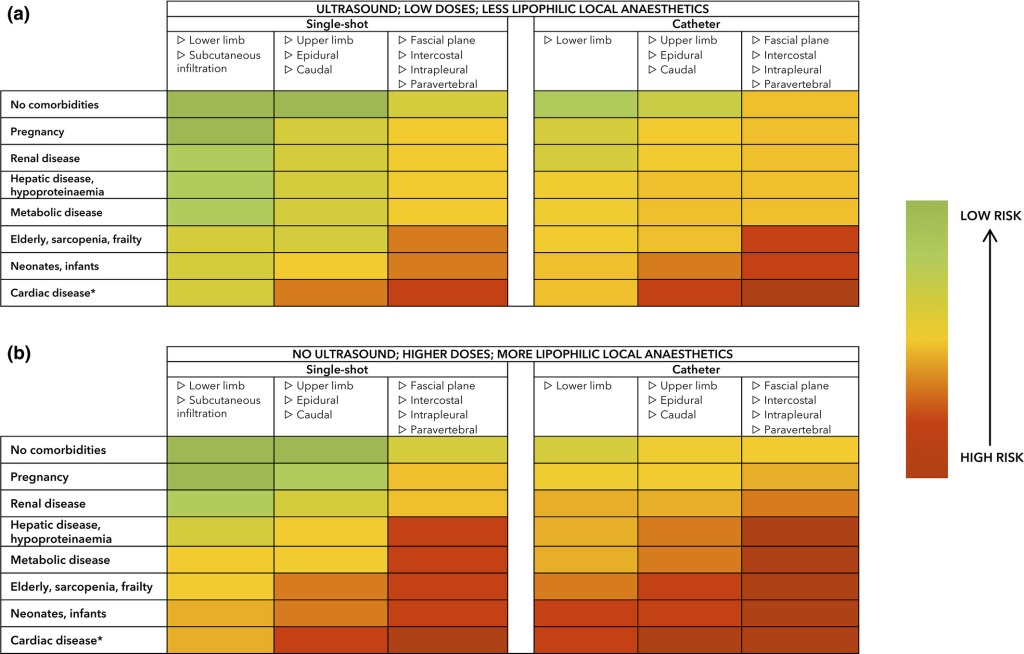 Figure 2. Risk of local anaesthetic systemic toxicity depending on anaesthetic technique and patient factors. From Macfarlane et al. (2021).A final paper focusing on safety comes from Levy and Lirk, who describe the challenges and considerations for regional anaesthesia in patients with diabetes. Key characteristics of this patient population, include a higher current threshold for peripheral nerve stimulation; a tendency to prolonged conduction blockade; and lower local anaesthetic dose requirements. There is also concern over a higher risk of infection with both central and peripheral nerve blocks, emphasising the need for strict adherence to aseptic precautions.
Figure 2. Risk of local anaesthetic systemic toxicity depending on anaesthetic technique and patient factors. From Macfarlane et al. (2021).A final paper focusing on safety comes from Levy and Lirk, who describe the challenges and considerations for regional anaesthesia in patients with diabetes. Key characteristics of this patient population, include a higher current threshold for peripheral nerve stimulation; a tendency to prolonged conduction blockade; and lower local anaesthetic dose requirements. There is also concern over a higher risk of infection with both central and peripheral nerve blocks, emphasising the need for strict adherence to aseptic precautions.
Efficacy
The contributions of regional anaesthesia to improved care in specific patient populations is highlighted in several articles. Regional anaesthesia has been relatively under-utilised in paediatric practice, but several factors have driven a recent resurgence, including concerns over the effects of general anesthesia on cognitive development in younger children. Heydinger et al. also point to several innovations that have improved efficacy in this setting, including fascial plane techniques such as quadratus lumborum and erector spinae plane blocks.
In contrast, regional anaesthesia is well-established in the obstetric setting, but there continues to be debate over the role of fascial plane blocks versus intrathecal opioids in post-caesarean analgesia. Sultan et al.summarise the latest evidence and offer suggestions on how we can rationally incorporate peripheral nerve blocks into our daily practice.
In another article, Dockrell and Buggy describe the current role of regional anaesthesia within the context of onco-anaesthesia. The pathophysiology of cancer recurrence is incredibly complex and multi-faceted, which makes it difficult to tease out the specific contribution of any one factor in peri-operative care. The evidence is just starting to accumulate and, in the meantime,, the authors point to the other advantages that regional anaesthesia may have on enhancing patient recovery and make a good case for its continued investigation and use.
Regional anaesthesia may also have an impact on chronic postoperative pain, a condition that affects between 5–50% of patients. Like cancer recurrence, the aetiology of chronic postoperative pain is complex and incompletely understood (Fig. 3). Nevertheless, as Chen et al. point out, regional anaesthesia remains an essential component of the “multimodal analgesic toolbox”. Procedure, patient or technique-specific approaches to peri-operative care may be required to have a real impact, but further evidence is needed before definitive recommendations can be made.
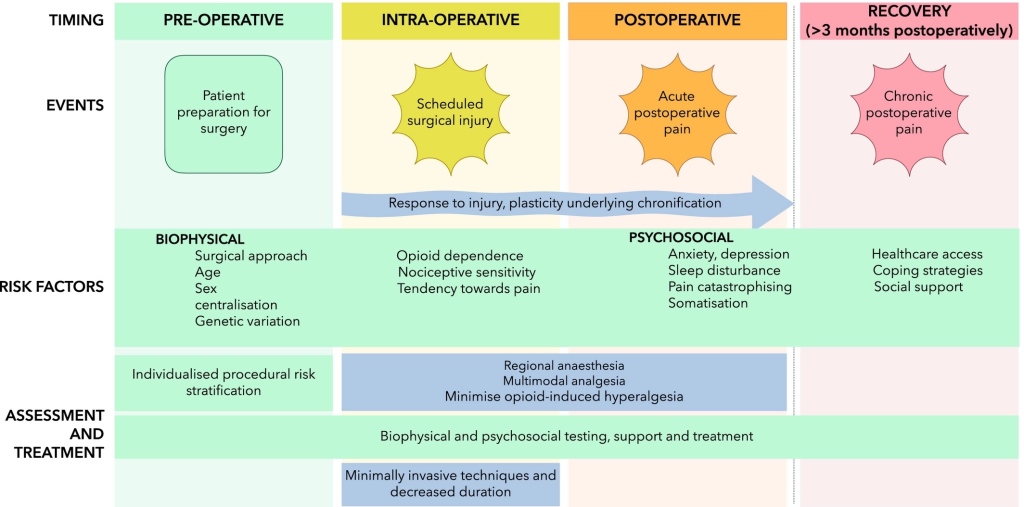 Figure 3. Timing, events and risk factors contributing to the development of chronic postoperative pain; with assessment and treatment to prevent chronic postoperative pain. From Chen et al. (2021).
Figure 3. Timing, events and risk factors contributing to the development of chronic postoperative pain; with assessment and treatment to prevent chronic postoperative pain. From Chen et al. (2021).Quality
One of the challenges of regional anaesthesia is determining its overall benefit to healthcare. Johnston and Turbitt argue that successful regional anaesthesia should be judged in four domains : patient‐centred, population‐centred, healthcare‐centred and training‐centred outcomes. Each of these contain several metrics that must be quantified, analysed and improved upon for patient benefit. This landmark paper serves to refocus our exploration of regional anaesthesia on outcomes that matter, with implications for both research activity and clinical implementation.
With respect to healthcare- and population-centred outcomes, Hamilton et al. report the results of a systematic review of the quality indicators that have been used in regional anaesthesia studies. Using a Donabedian framework, they sought structure (administrative settings supporting care provision), process (the act of providing care) and outcome (patient recovery, restoration of function or survival) indicators. Predictably, the latter was most commonly reported, with only 6% and 18% of studies reporting structure or process indicators, respectively.
The importance of imparting regional anaesthesia skills to all trainees has already been mentioned. Ramlogan et al. highlight contemporary training methods in regional anaesthesia, in particular the use of modern technologies such as web-based learning, wearable devices and virtual reality systems. The effectiveness of these novel methods must be tracked using the appropriate training-centred outcomes.
Finally, McCombe and Bogod tackle the challenging subject of risk, consent and complications in regional anaesthesia. The significance of how we communicate risk is described, and how this communication leads to appropriate and legally sound consent, particularly in the post-Montgomery era.
Innovations
Both clinical and technological innovations share the spotlight in this issue. One of the foremost clinical innovations in recent years is the development of chest wall blocks. The current state of the art and future directions for this class of blocks are summarised by Chin et al. Pharmacological adjuncts for peripheral and central neuraxial blocks have also been an area of intense clinical and research interest. Desai et al. conduct a deep dive into these adjuncts that among other things, may leave many readers convinced that intravenous dexamethasone has effects beyond anti-emesis and therapy for COVID-19.
The rapid pace of technological advancement and its application to regional anaesthesia are described in a complementary pair of articles. McKendrick et al. provide fascinating insights on how artificial intelligence and robotics will not only support clinical practice but potentially be the standard of practice in their own right. Finally, safe and successful regional anaesthesia has been described as primarily a matter of “getting the right drug into the right place”. Dr McLeod describes the exciting prospects for solving this perennial problem with technologically-enhanced needle-tip tracking in ultrasound-guided regional anaesthesia.
Conclusion
The papers in this special issue provide a broad overview of the current state of regional anaesthesia. The hope is that all anaesthetists, and not just the enthusiasts, will find value in the content. More importantly, we hope that it will spur the continued expansion in provision of regional anaesthesia to our patients. There is a tremendous opportunity to improve delivery of healthcare and patient outcome, and we invite readers to join us as we take the next step forward on the path to regional anaesthesia excellence and access for all.
Leave a Reply
You must be logged in to post a comment.