
Author: Michael Vlessides
Anesthesiology News
A higher body mass index (BMI) is a significant predictor of 30-day hospital readmission after ambulatory open hernia repair, a study has found. The investigators’ regression model indicated that a BMI of 45.7 kg/m2 could be used as a threshold value for deciding whether obese patients should undergo the surgery as inpatients or outpatients.
“Obesity is highly prevalent in the [United States] and many other countries, and more and more patients show up for ambulatory surgery with large BMIs,” said Eric Rosero, MD, an assistant professor of anesthesiology and pain management at UT Southwestern Medical Center, in Dallas. “We know that increasing obesity is a predictor of complications, but the key question here is when to say, ‘Stop, this patient is not a good candidate for outpatient surgery and should stay at least one day in the hospital.’”
With this in mind, the researchers sought to determine the adjusted cutoff value of BMI that is associated with an increased likelihood of 30-day hospital readmission after ambulatory surgery, using open hernia repair as the index procedure.
Dr. Rosero and his co-investigator Girish Joshi, MD, MBBS, used data from the American College of Surgeons’ National Surgical Quality Improvement databases for 2012 to 2014, to identify adult patients undergoing elective, ambulatory hernia repair (inguinal, femoral or ventral). The study’s primary outcome was the occurrence of any hospital readmission within 30 days of the operation.
As Dr. Rosero reported at the 2018 annual meeting of the International Anesthesia Research Society (abstract AMB2), a total of 86,538 ambulatory open hernia repair procedures were identified. The median BMI (interquartile range) of the cohort was 27.5 (24.5-31.4) kg/m2. “Only 28% of the patients had a BMI below 25,” Dr. Rosero said. “Approximately one-third were overweight, and about one-third or more had some degree of obesity.” The overwhelming majority of patients (75.1%) were men.
The analysis revealed that the crude 30-day hospital readmission rate was 1.8%. The unadjusted 30-day readmission rate was found to increase significantly with rising BMI (P<0.0001) (Table).
| Table. Hospital Readmission by BMI Value | |
| BMI, kg/m2 | 30-Day Readmission Rate, % |
|---|---|
| ≤25 | 1.55 |
| 25 to <30 | 1.56 |
| 30 to <40 | 2.08 |
| 40 to <50 | 2.86 |
| 50 and over | 3.98 |
| BMI, body mass index | |
After adjusting for age and probability of morbidity, multivariate analysis revealed that BMI remained a significant predictor of 30-day readmission (odds ratio [OR], 1.011; 95% CI, 1.003-1.019; P<0.0001) (Figure). “What this means is that each time we increase the BMI value by five points, there is an increased risk of readmission by about 6%,” Dr. Rosero explained.
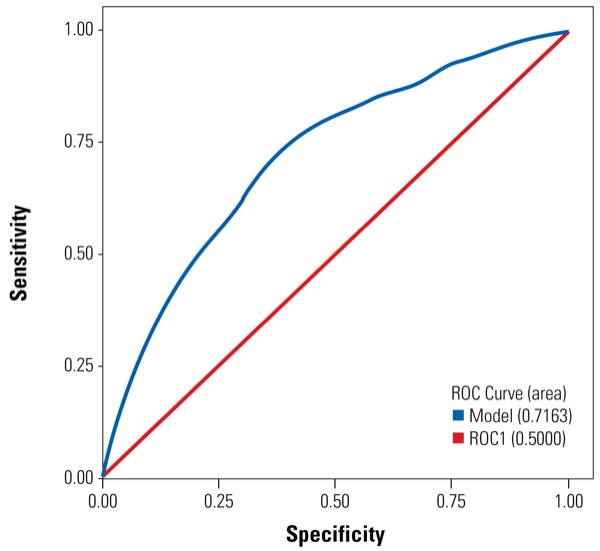
The BMI threshold that was associated with an increased likelihood of 30-day hospital readmission was found to be 45.7 kg/m2. “In doing this analysis,” Dr. Rosero said, “we found a sensitivity of 60.4% and a specificity of 71.4%.” The area under the curve for the regression model was 0.71, indicating fair accuracy. “This is OK,” he said, “but not perfect.”
Given the modest discriminating ability of the model, Dr. Rosero recommended considering more than just BMI when deciding which patients are the best candidates for outpatient surgery. “According to our model, a cutoff value of 45.7 could be used as a potential threshold for selecting patients for outpatient surgery,” he concluded. “Nevertheless, since the discriminating ability of the model was not perfect, we have to see each patient individually according to other factors to determine whether the patient is a good candidate or not.”
Roman Schumann, MD, a professor of anesthesiology at Tufts University School of Medicine and Tufts Medical Center, in Boston, reminded his colleagues that although BMI is easily obtained and attractive for studies relating to obesity, the measure is less than ideal for any obesity-related risk assessment. “Hence, the determination of limits that reliably indicate the appropriateness of a given obese patient for outpatient procedures has been a challenge.
“The strength of this study is in its large sample size,” Dr. Schumann continued. “Not too surprisingly, the risk of 30-day readmission following a routine outpatient surgery increases with the degree of obesity. As perioperative clinicians have adapted to the obesity epidemic, the temptation to accept greater degrees of obesity for ambulatory procedures is a reality, and the need to have accepted threshold parameters is ever more urgent.
“A BMI of 45 as a guide may well be suitable, as this seems to be a limit where the human physiology significantly changes for the worse, particularly in the respiratory domain,” he added. “In concert with additional clinical parameters, this could be a very good benchmark to include in decision making. It would be great to have additional information regarding type of anesthesia, comorbidities and reasons for readmissions when a final analysis of these data becomes available.”
Leave a Reply
You must be logged in to post a comment.