
Authors: Mike Charlesworth and Andrew Klein
#theanesthesiablog
Despite several published guidelines recommending the use of peri-operative checklists, there is a paucity in reporting team adherence to checklist use. This new 5-year audit from Fuchs et al. aimed to report the adherence of anaesthesia providers to an anaesthesia pre-induction checklist. The checklist was to be undertaken before induction of anaesthesia and it included components related to: equipment; the patient; communication; and feasibility. They included 95,946 anaesthesia procedures with airway management, with overall completion in almost 60% of all procedures. They showed a 4.5% increase in the annual adherence rate (Fig. 1). Factors influencing adherence included the type of anaesthesia, variability between anaesthesia teams for different surgical specialities and urgent and daytime procedures. The checklist was used more frequently in the operating theatre, for non-emergency procedures and during daytime working hours. Saxena et al. draw comparisons with the well-known plane landing on the Hudson. Although well-designed checklists aim to reduce human error, they are only effective if implemented effectively. Regular audits like those reported by Fuchs et al. are useful to study patterns and reasons for non-compliance.

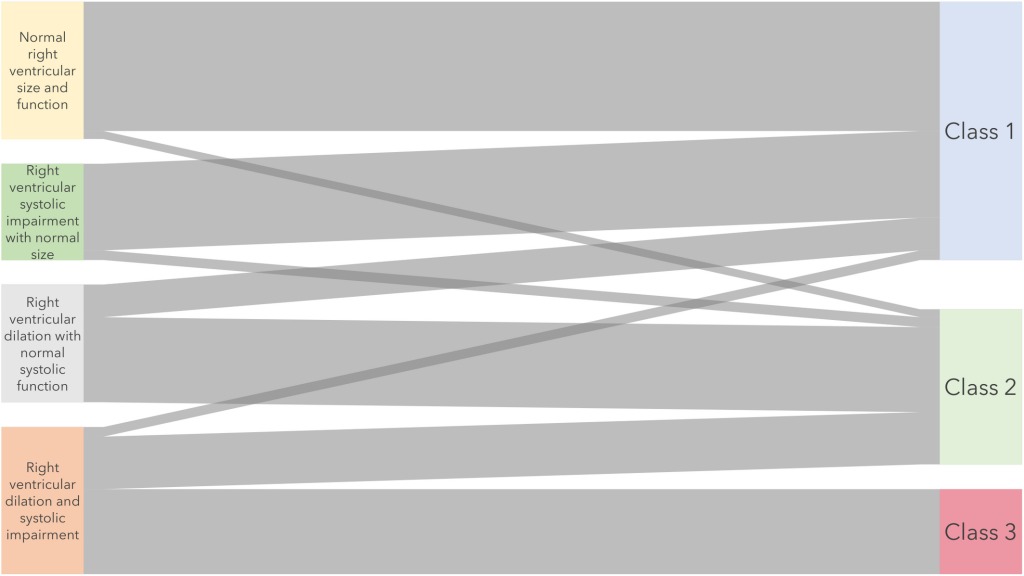
During the early pandemic, there was much anecdotal evidence of a high incidence of right ventricular failure in ICU patients with COVID-19 and a suggestion of an association with mortality. Chotalia et al. undertook a retrospective observational study of 508 patients with COVID-19 pneumonitis of whom 305 (60%) underwent echocardiography. They identified three classes of patients from echocardiographic and clinical variables (Fig. 2). These subphenotypes had distinct clinical and outcome characteristics. McCall et al. add to this with their COVID-RV prospective study of 121 patients, of whom 112 (91%) underwent imaging. They found that the prevalence of right ventricular dysfunction was 6% and this was associated with a mortality of 86%, in contrast to 45% in those without right ventricular dysfunction. The associated editorial discusses the issues around imaging the right ventricle and determining when there is a problem. The key take-home message though is that we need to get better at echocardiography in ICU, perform it more regularly and use it to demonstrate, treat and monitor right ventricular injury earlier than we do currently.
These new guidelines from the British Heart Rhythm were extremely well received on social media. Recommendations are provided around peri-operative pacemaker checking, functioning, deactivation and follow up. Before their initial release in 2016, there were no specific UK guidelines on this topic. Whilst much of the new update is based on expert opinion due mainly to a lack of trial date, anaesthetists are seeing more patients with cardiac implantable devices and the recommendations provided are of relevance to all. Two editorials feature in this issue that are associated with papers published earlier in the year. First, Ruslan and Smith make an argument for shorter and safer pre-operative fasting times in children. Afterall, the incidence of aspiration during anaesthesia for children in the associated study was approximately 0.1% and more than half of those that aspirated had an uneventful outcome. Second, Bailey and George ask, is further peri-operative research necessary for patients undergoing colorectal cancer surgery? They suggest that future trials should focus on homogenous surgery, a specific TIVA technique, a fixed intrathecal dose of opioid and patient outcome measures that matter.
Elsewhere we have a retrospective cohort study of ultrasound-guided caudal blockade and sedation for paediatric surgery and a randomised controlled feasibility trial of a clinical protocol to manage hypotension during major non-cardiac surgery. Finally, this meta-analysis from Pivetta et al. finds that the presence of obstructive sleep apnoea is associated with an almost two-fold increased risk of postoperative complications. There was also moderate certainty for patients with obstructive sleep apnoea having increased risk of cardiovascular complications (OR 1.56), atrial fibrillation (OR 1.74), respiratory complications, neurological complications, hospital and ICU re-admission postoperatively (Fig. 3).

Leave a Reply
You must be logged in to post a comment.