
Author: Ethan Covey
Anesthesiology News
Most children who undergo MRI while under anesthesia experience hypothermia at some point during the procedure, according to a new study.
However, those who became hypothermic did not show an increased rate of perianesthesia complications or longer PACU length of stay (LOS).
“Temperature derangements can cause several harmful physiological responses in pediatric patients undergoing anesthesia,” said Jessica Cronin, MD, an anesthesiologist in the Department of Anesthesiology, Pain and Perioperative Medicine at Children’s National Health System, in Washington, D.C. “Prior literature had shown increased risk for hypothermia and hyperthermia for pediatric patients that require anesthesia to undergo MRI. With the introduction of MRI-compatible continuous temperature monitoring, we hoped to get a better understanding of temperature trends for anesthetized pediatric patients undergoing MRI.”
Dr. Cronin and her colleagues used temperature information to improve the management of these patients. The researchers evaluated 285 pediatric outpatients who underwent anesthesia before undergoing MRI. All patients were less than 8 years of age (Table 1).
| Table 1. Demographics | |
| Characteristic | N=285 |
|---|---|
| Age (years), mean (SD) | 3.6 (2.1) |
| Sex, n Male Female | 168 (58.9%) 117 (41.1%) |
| Weight (kg), mean (SD) | 16.4 (6.5) |
| Pre-MRI temperature, mean (SD) | 36.5 (0.7) |
| Intra-scan temperature, mean (SD) | 35.7 (0.8) |
| Intra-scan temperature, median (SD) | 35.7 (0.8) |
| Lowest intra-scan temperature, mean (SD) | 35.2 (1.1) |
| Post-MRI temperature, mean (SD) | 36.3 (0.3) |
| Hypothermia, n Yes No | 179 (62.8%) 106 (37.2%) |
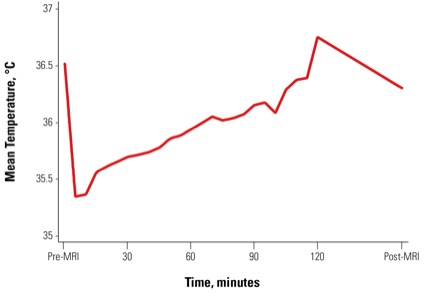
Hypothermia was defined as a mean intra-scan body temperature less than 36° C, and hyperthermia was defined as greater than 38° C. The patient’s temperature was noted pre-MRI, and at 30, 60, 90 and 120 minutes post-MRI (Figure).
The associations between hypothermia and length of anesthesia, age, sex, weight, heart rate and preoperative temperature were compared via an unpaired t test and chi-square test. Additionally, the relationship between PACU LOS with hypothermia, length of anesthesia, sex, age, propofol dose, and pre- and postoperative temperatures was explored.
Upon completion of the study, 67% of patients exhibited hypothermia at some point during MRI, whereas hyperthermia occurred in none of the children. Most incidences of hypothermia occurred early in the scan.
“We found that hypothermia was significant, particularly during anesthesia induction and prior to the initiation of the MRI scan,” Dr. Cronin said. “The scanning environment is typically kept cool (18° C±3° C) with a low humidity (45%±15%), and heat loss to the surrounding environment typically occurs after induction of anesthesia. Subsequently, patients experience an increase in body temperature during the MRI scan secondary to MR radiofrequency heating.”
While common, hypothermia did not have an effect on PACU LOS, even after adjusting for confounding variables (Table 2). However, the researchers stressed the importance of monitoring hypothermia, particularly in the most vulnerable patients.
| Table 2. Associations With PACU Length of Stay | ||
| Variable | PACU Duration, minutes | |
|---|---|---|
| Coefficient (95% CI) | P Value | |
| Anesthesia duration, minutes | 0.12 (0.02-0.23) | 0.02 |
| Age | 1.94 (0.64-3.25) | 0.004 |
| Sex (Female) | 1.83 (–3.94-7.60) | 0.53 |
| Weight | 0.78 (0.35-1.21) | <0.001 |
| Propofol dose, mg/kg | 0.13 (–0.01-0.26) | 0.08 |
| Preoperative temperature | –3.34 (–12.48-5.8) | 0.47 |
| Postoperative temperature | –3.73 (–14.83-7.38) | 0.51 |
“While our study did not identify any perianesthesia complications associated with hypothermia, the smallest and sickest patients may be at increased risk to develop hypothermia and its complications,” Dr. Cronin added.
“Based on our findings, interventions for these patients should be focused on maintaining normothermia during the anesthesia induction and prior to initiation of the MRI scan. MRI-compatible continuous temperature monitoring is also instrumental for managing temperature for these anesthetized patients” (Table 3).
| Table 3. Ways to Reduce Heat Loss or Increase Warming In Children Undergoing MRI With Sedation |
| Increase ambient temperature in induction area |
| Use of heat lamps, heated blankets, chemical warmers in induction area |
| Minimize exposure of child to ambient environment |
| Continuous axillary temperature measurement |
| Use of chemical warmers |
| Minimize exposure of child to ambient environment |
| Turn off MRI fan, if possible |
For Dr. Cronin, further exploration of these high-risk populations would further elucidate any connection between hypothermia and complications.
“Our study was limited to outpatient pediatric patients, but it would be helpful to extend this effort to include more vulnerable populations who may be at higher risk for developing complications secondary to temperature derangements,” she said. “Further evaluation regarding effective methods to reduce the incidence of hypothermia would provide practical clinical guidance on how to maintain normothermia in these patients.”
The research was presented at the 2019 annual meeting of the Society for Pediatric Anesthesia/American Academy of Pediatrics.
Leave a Reply
You must be logged in to post a comment.