
Author: Michael Vlessides
Anesthesiology News
A Florida institution has devised an innovative approach to addressing the opioid crisis. Its new opioid therapy algorithm consolidates a host of recent guidelines and recommendations into a single guide that it hopes will assist physicians of all specialties in prescribing opioids safely and effectively.
“As we all know, the opioid crisis has contributed to hundreds of thousands of deaths over the past 20 years or so,” said Jason D. Lefkof, DO, an anesthesiology resident at the University of Miami Miller School of Medicine. “So we decided to implement an algorithm to help medical providers optimize their treatment and care plans to address this.”
In response to publication of the CDC guideline, a variety of relevant societies—including the American Society of Anesthesiologists (ASA), American Academy of Pain Medicine, and American Society of Regional Anesthesia and Pain Medicine—published official position statements.
Despite the proliferation of these various statements, a chronic opioid therapy algorithm has yet to be published that can help clinicians of all specialties initiate and manage chronic opioid therapy for noncancer pain.
“We took all of these guidelines and recommendations and used them as a framework for an algorithm that we are in the process of implementing at the University of Miami, Jackson Memorial Hospital and the Miami VA,” Dr. Lefkof explained at the 2019 annual meeting of the International Anesthesia Research Society (abstract D128).
The algorithm begins with a thorough patient assessment and medical history; psychological and behavioral evaluation; physical examination; review of diagnostic studies; review of previous and current treatment modalities; drug history; and assessment of coexisting diseases and conditions. This assessment also includes appropriate drug testing and a baseline drug screen.
The patient assessment allows practitioners to determine whether the patient is suffering from acute pain, chronic cancer pain or chronic noncancer pain, which includes neuropathic, somatic or visceral pain syndromes.
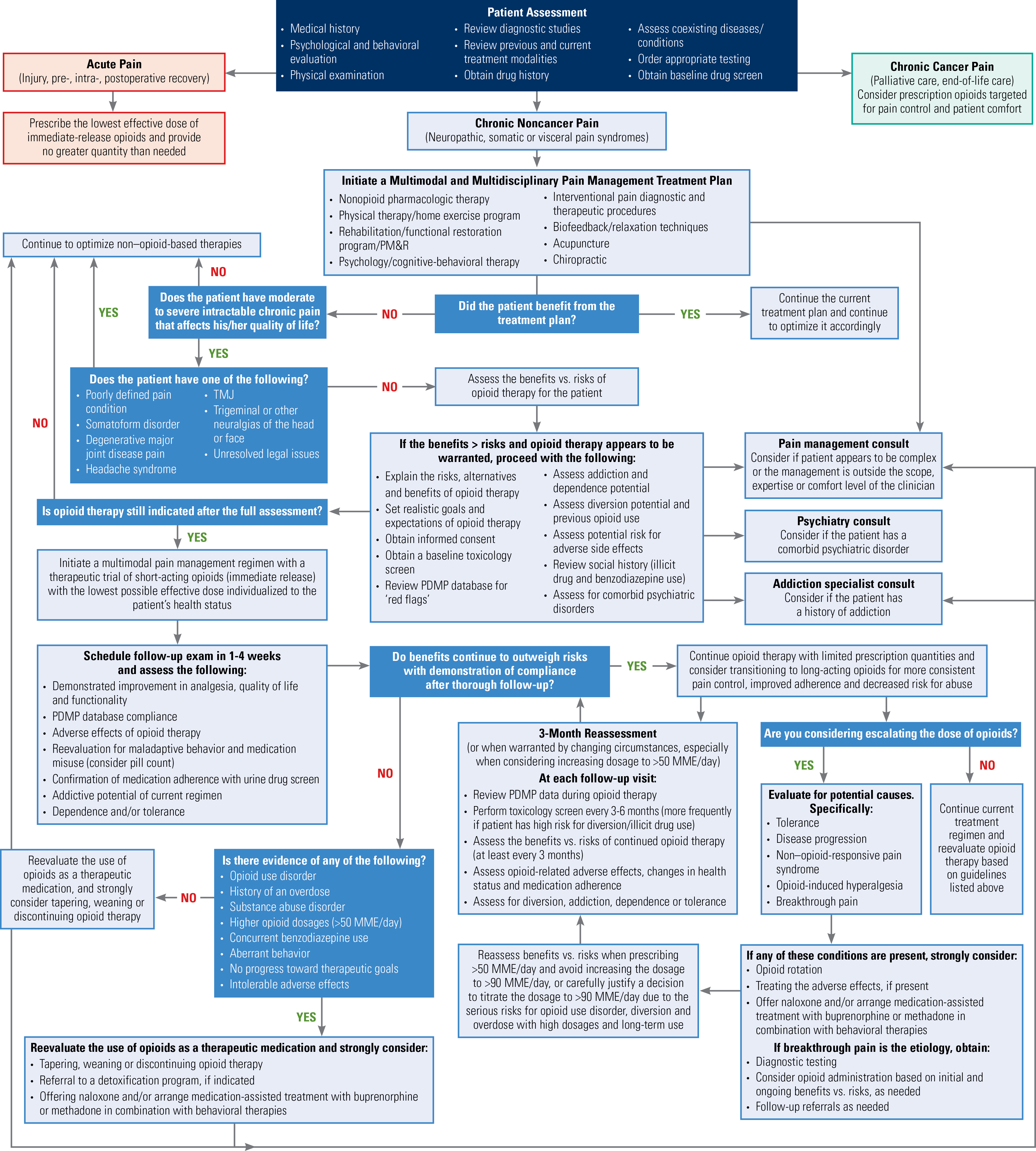
Once it has been determined that the patient has chronic noncancer pain, the algorithm recommends initiation of a multimodal, multidisciplinary pain management treatment plan.
“We really wanted to optimize multimodal, multidisciplinary care as the primary focus for chronic noncancer pain patients before initiating or supplementing their pain management regimen with opioid therapy,” Dr. Lefkof said. “We feel patients would benefit from this first, based on what the CDC and other societies have recommended, and if opioids are indicated we wanted to ensure they are prescribed safely with the appropriate follow-up and clinical considerations.”
Understandably, this uses a variety of approaches, including nonopioid pharmacologic therapy; physical therapy and home exercise; rehabilitation/functional restoration; psychology and cognitive-behavioral therapy; interventional pain diagnostic and therapeutic procedures; biofeedback and relaxation techniques; acupuncture; and chiropractic therapy.
“If the primary care physicians and surgeons are not able to provide these options as their first line of treatment, patients can be referred to a pain management specialist,” Dr. Lefkof noted.
If the patient benefited from the multimodal therapy, it should be continued. If not, clinicians need to assess whether the patient is suffering from chronic intractable pain.
“Here, the ASA identified a variety of poorly defined conditions that would not be amenable to opioid therapy and require optimization of nonopioid therapy,” Dr. Lefkof explained.
These conditions include a poorly defined pain condition; somatoform disorder; degenerative major joint disease; headache syndromes; temporomandibular joint disorders; neuralgias of the head or face; and unresolved legal issues.
- Explain the risks, alternatives and benefits of opioid therapy.
- Set realistic goals and expectations of opioid therapy.
- Obtain informed consent.
- Obtain a baseline toxicology screen.
- Review the prescription drug monitoring program (PDMP) database for so-called “red flags.”
- Assess addiction and dependence potential.
- Assess diversion potential and previous opioid use.
- Assess the potential risk for adverse side effects.
- Review social history (illicit drugs and benzodiazepine use).
- Assess for comorbid psychiatric disorders.
“And if, after all that, opioid therapy is still indicated, then you would start short-acting opioids at the lowest possible dose,” he added.
A follow-up appointment is scheduled in one to four weeks, at which patients are assessed for demonstrated improvements in analgesia, quality of life and functionality; PDMP database compliance; adverse effects of opioid therapy; reevaluation for maladaptive behavior and medication misuse; confirmation of medication adherence with urine drug screening; addictive potential of the current regimen; and dependence and/or tolerance.
If patients do not demonstrate any maladaptive behaviors and the benefits of opioid therapy continue to outweigh its risks, then clinicians can continue opioid therapy with limited prescription quantities. Along with this, clinicians should consider transitioning to long-acting opioids for more consistent pain control, improved adherence and decreased risk for abuse.
“This algorithm helps to address chronic noncancer pain and optimize treatment plans for patients presenting at the initial visit, as well as for those who are well-established pain patients,” Dr. Lefkof said.
These individuals should be reassessed at three months. At this appointment, one of the most important factors is noting whether the patient’s dose has escalated beyond 50 milligram morphine equivalents per day, which is the benchmark the CDC has identified as signaling higher risk.
“If you’re escalating the opioid dose beyond this, you should consider assessing for tolerance or other conditions that may need further workup,” Dr. Lefkof said. “And if at that point there’s evidence of opioid use disorder or aberrant behavior, then you would consider tapering, weaning or discontinuing opioid therapy; arranging for treatment plans comprising naloxone and/or buprenorphine or methadone; and consider referring them to a detoxification program with access to an addiction specialist who can help manage and prescribe them these medications.”
The algorithm offers clinicians an intuitive guide to prescribing opioids both safely and effectively for chronic noncancer pain, with a special emphasis on primary care.
“We are also interested in working collaboratively with other medical centers that would like to implement the algorithm, further measure patient outcomes, and help end the opioid crisis in our country,” he added.
“The ultimate goal is to help medical providers consolidate care and optimize treatment plans, with more responsible opioid prescribing practices and referrals, when needed.”
Overwhelming Visual Display
For Beth D. Darnall, PhD, an associate professor of anesthesiology, perioperative and pain medicine, and a principal investigator of the Stanford PCORI (Patient-Centered Outcomes Research Institute) Project on Opioid and Pain Reduction at Stanford University, in California, the new tool offers tangible potential benefits. “The algorithm provides an opioid medical decision-making guide that represents the consolidated consensus statements, guidelines and positions of multiple national medical and professional pain societies,” Dr. Darnall said. “It also emphasizes risk/benefits and multimodal approaches,” she added.
Nevertheless, as Dr. Darnall explained, the algorithm is not without its weaknesses, beginning with adding detail and brief guidance regarding opioid tapering. “Simply listing ‘tapering’ and ‘discontinuation’ implies this is simply implemented,” she said. “The recent FDA caution and CDC clarification statement both caution against forced and rapid opioid tapering.”
As Dr. Darnall explained, opioid reduction requires at least attention to medical decisions, processes and protocol, as does opioid initiation and management. This, she said, will help prevent iatrogenic harms from “de-prescribing.”
“The tool could be strengthened by emphasizing these important points and cautions regarding opioid reduction,” she said.
Additionally, Dr. Darnall said the algorithm does not account for patient accessibility to nonopioid pain treatments. She also mentioned the potential for an electronic format with branching logic, which “could facilitate practical use of this clinical decision tool and eliminate an overwhelming visual display.”
Dr. Darnall noted that these suggestions could possibly enhance a potentially important and useful tool for opioid-prescribing clinicians.
Leave a Reply
You must be logged in to post a comment.