

Introduction
We report the use of multiple regional anesthesia techniques to provide analgesia for a patient with thoracic outlet syndrome (TOS), who presented for a right first rib resection and whose opioid use needed to be minimized due to the patient’s history of postoperative nausea and vomiting. We placed a right-sided T3-T4 paravertebral catheter for continuous infusion of a local anesthetic solution and performed right-sided interscalene brachial plexus and superficial cervical plexus nerve blocks to address multiple sources of pain: the right first rib resection (T1 spinal nerve root), the anterior scalene muscle and a horizontal infraclavicular skin incision in the C4-C5 dermatomal region, respectively.1 All regional anesthesia techniques were performed prior to incision. This combined regional anesthesia technique provided excellent analgesia intraoperatively and postoperatively with minimal narcotic requirement, near-complete analgesia, and no postoperative nausea and vomiting.
Discussion
TOS is a constellation of symptoms that arise from the compression of the neurovascular bundle by various structures in the region superior to the first rib and posterior to the clavicle.2,3 TOS can be subdivided into three categories: 1) neurogenic, involving the compression of the brachial plexus; 2) venous, which is a result of subclavian vein compression; and 3) arterial, caused by compression of the subclavian artery.2,3 Neurogenic TOS accounts for 95% of cases, with 3% and 1% of the cases stemming from vascular and arterial causes, respectively.3
Surgical management of TOS involves resection of the first rib and other structures causing compression of the surrounding tissue.2,3 Surgical approaches are usually supraclavicular, infraclavicular or transaxillary.2,3 One of the major concerns is postoperative pain, which causes significant morbidity and is one of the limiting factors contributing to delayed discharge of these patients.
Regional anesthesia may provide superior postoperative pain control than other modalities, such as IV opioids.4,5 A paravertebral technique may offer similar analgesia with fewer side effects, such as hypotension, compared to thoracic epidural analgesia.4,5
Case Report
DT is a 49-year-old woman with a history of smoking and oral contraceptive use, who presented for resection of her right first rib, after being diagnosed three months earlier with right upper extremity deep vein thrombosis. A CT scan of the right upper extremity confirmed the diagnosis of TOS. Preoperatively, her primary concerns were her postoperative pain management, as well as severe nausea and vomiting with opioid use.
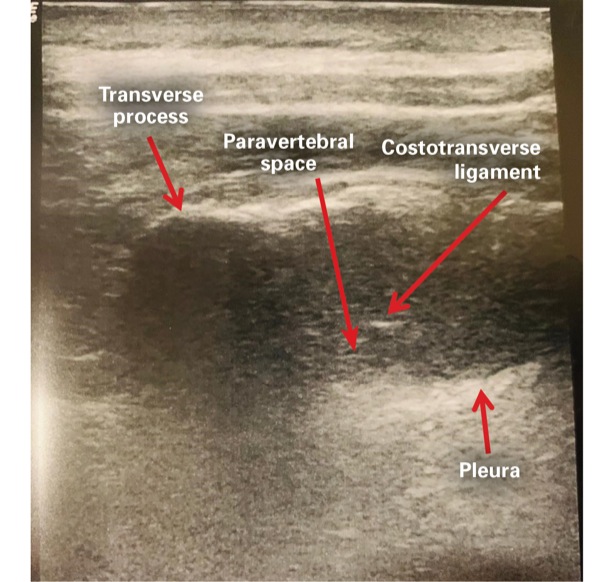
We obtained consent for a paravertebral catheter, an interscalene brachial plexus block, a cervical plexus block and general anesthesia (Figures 1-3). She received 2 mg of midazolam and 100 mcg of fentanyl intravenously for sedation during the regional anesthesia procedures. She was placed in the sitting position for placement of the paravertebral catheter under ultrasound guidance, located at the T3-T4 interspace, using an 18-gauge Touhy needle. A 20-gauge catheter was advanced into the paravertebral space, at a depth of 5 cm, sutured at the skin.
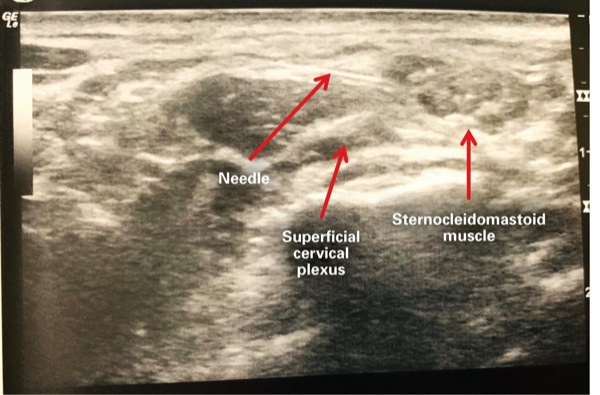
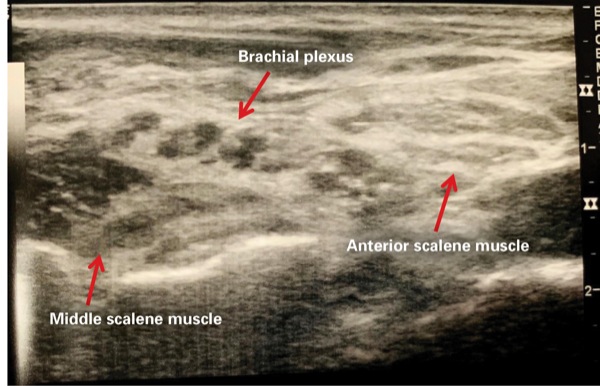
We injected 15 mL of 0.25% bupivacaine into the T3-T4 paravertebral space and threaded a perineural catheter with the use of saline and 5 mL of 1% lidocaine for volume expansion of the paravertebral space in order to enhance catheter passage and visualization via ultrasound guidance. We then performed right-sided interscalene brachial plexus and cervical plexus blocks, with 20 mL of 0.25% bupivacaine with epinephrine 1:200,000, via ultrasound guidance, using a 22-gauge 5-cm echogenic needle.
DT received a total of 150 mcg of fentanyl intravenously, which was administered during placement of the regional nerve blocks. She did not receive any further IV opioids during her hospitalization. On postoperative day 1, her highest pain score was 1 of 10, which was treated with 400 mg of ibuprofen and 0.1% bupivacaine via the T3-T4 right paravertebral catheter, which was infused at 6 mL per hour. We removed the paravertebral catheter on postoperative day 2. She received one tablet of hydrocodone-acetaminophen 5/325 mg and gabapentin 100 mg orally for a pain score of 1 of 10 and was discharged to home.
We called the patient on postoperative day 3, and she denied pain or neurologic symptoms and was very pleased with her hospital stay.
Conclusion
We report an alternative analgesic method for patients with TOS undergoing first rib resection. This combination of regional anesthesia techniques (paravertebral catheter, interscalene and superficial cervical plexus nerve blocks) resulted in excellent analgesia. Further research must be conducted to evaluate the efficacy and applicability of these regional anesthesia techniques in patients presenting for similar procedures.
The authors reported no relevant financial disclosures. The corresponding author is Dr. Suneel, at fnu.suneel@bhs.org.
References
- Gray H. Anatomy of the Human Body. Philadelphia, PA: Lea & Febiger; 1918. www.bartleby.com/ 107/ . Accessed July 12, 2019.
- Sanders RJ, Hammond SL, Rao NM. Diagnosis of thoracic outlet syndrome. J Vasc Surg. 2007;46(3):601-604.
- Foley JM, Finlayson H, Travlos A. A review of thoracic outlet syndrome and the possible role of botulinum toxin in the treatment of this syndrome. Toxins (Basel). 2012;4(11):1223-1235.
- Yeying G, Liyong Y, Yuebo C, et al. Thoracic paravertebral block versus intravenous patient-controlled analgesia for pain treatment in patients with multiple rib fractures. J Int Med Res. 2017;45(6):2085-2091.
- Malekpour M, Hashmi A, Dove J, et al. Analgesic choice in management of rib fractures: paravertebral block or epidural analgesia? Anesth Analg. 2017;124(6):1906-1911.
Leave a Reply
You must be logged in to post a comment.